Understanding Inflammatory Spondylopathy: Symptoms, Causes, and Treatment starts with one key fact: this is a pattern of spinal and sacroiliac joint inflammation that usually causes stiffness, especially in the morning, more than simple strain. If you want to know what is inflammatory spondylopathy, how it differs from routine back pain, and which conservative treatments may help, the answer usually involves a focused exam, movement-based rehab, and care that matches the source of irritation in the spine, pelvis, and surrounding soft tissue.
What Is Inflammatory Spondylopathy?
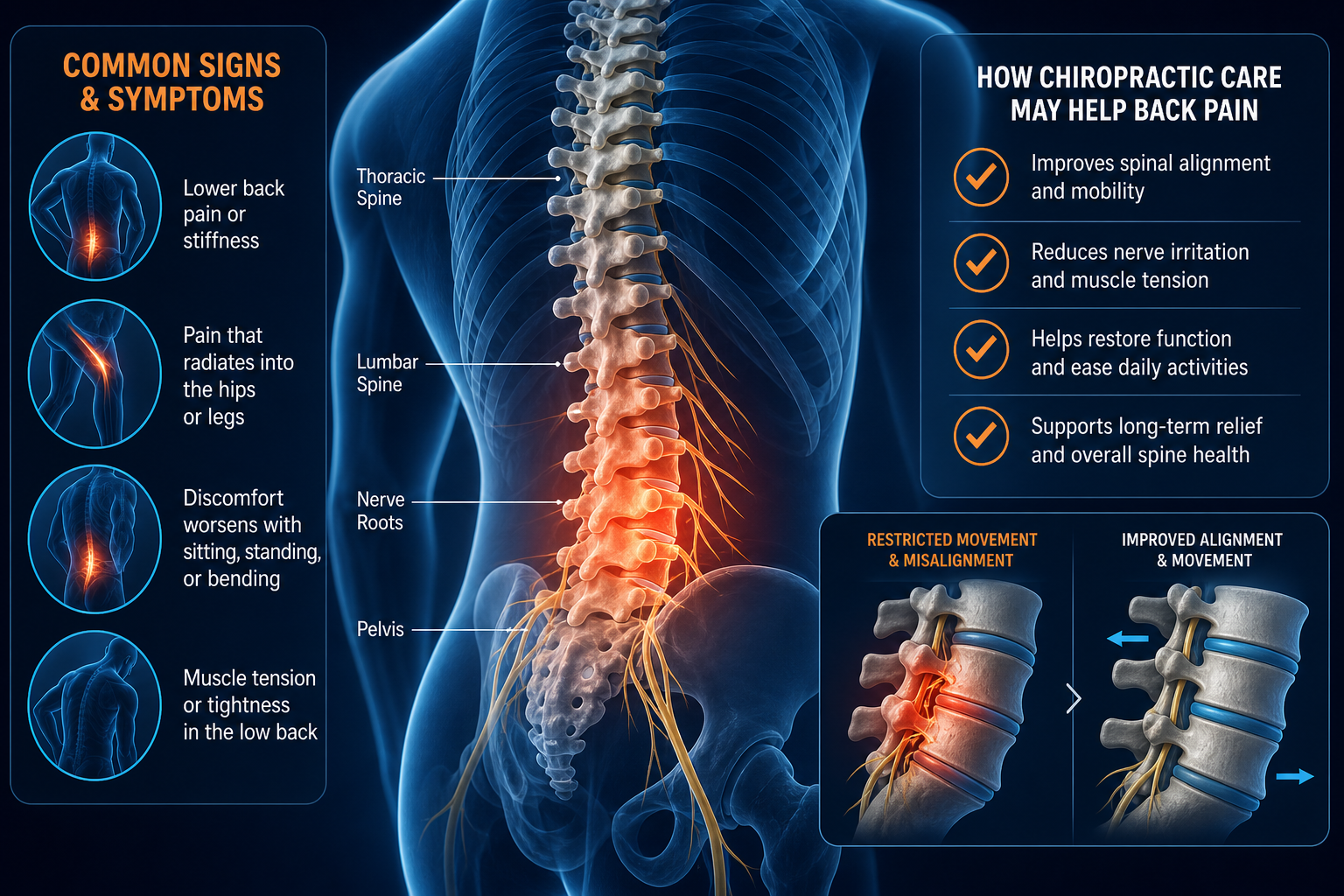
Inflammatory spondylopathy is a broad term used for inflammatory conditions that affect the spine, most often the sacroiliac joints, lumbar spine, and sometimes the thoracic spine or cervical spine. The word “spondylo” refers to the spine. “-pathy” means a disorder or disease process. In plain language, this means your back pain may be driven less by overuse of muscles and more by inflammation around spinal joints, ligaments, and the sites where tendons attach to bone.
This pattern often overlaps with conditions in the spondyloarthritis family. A provider may suspect it when back stiffness lasts more than 30 minutes in the morning, symptoms improve after movement, and pain is not fully explained by a recent lift, twist, or fall.
Structures commonly involved
- Sacroiliac joints at the base of the spine
- Facet joints between vertebrae
- Interspinous ligaments and surrounding connective tissue
- Hip flexors and gluteal muscles, which often tighten secondarily
Inflammatory spinal pain is not the same as nerve compression, although both can coexist. If your symptoms travel down the leg, compare that pattern with sciatica treatment and pain patterns because radiating symptoms may point to a different or additional problem.
Research on inflammatory back pain patterns commonly notes onset before age 45, gradual onset, morning stiffness, and improvement with activity rather than rest.
How does inflammatory back pain differ from mechanical back pain?
Inflammatory back pain vs mechanical back pain usually comes down to timing, behavior, and response to movement. Mechanical pain often flares after load, prolonged bending, awkward lifting, or sudden rotation. Inflammatory pain tends to build gradually, feel worse after inactivity, and ease as your joints warm up.
Feature Inflammatory Back Pain Mechanical Back Pain Onset Gradual, often over weeks to months Often linked to a specific strain or overload Morning stiffness Common, often 30-60 minutes or longer Usually brief Effect of rest May feel worse after rest Often improves with short rest Effect of movement Typically improves with gentle activity May worsen with repeated loading Night pain Can wake you in the second half of the night Less typical unless position-dependent Typical timeline Persistent for 3 months or longer Often improves within 2-6 weeksA stiff lower back in morning is one of the clearest clues. So is pain that improves after a walk, mobility drill, or hot shower.
Practical clues you can notice at home
- You loosen up after 10-20 minutes of moving.
- Sitting still for long periods makes the back and hips feel tighter.
- The ache may center near the dimples of the low back, where the sacroiliac joints sit.
- You may also notice reduced chest expansion or mid-back rotation.
Not every persistent back ache is inflammatory. Tight erector spinae, weak gluteus medius, or poor hip hinge mechanics can mimic it. That is why a structured exam matters.
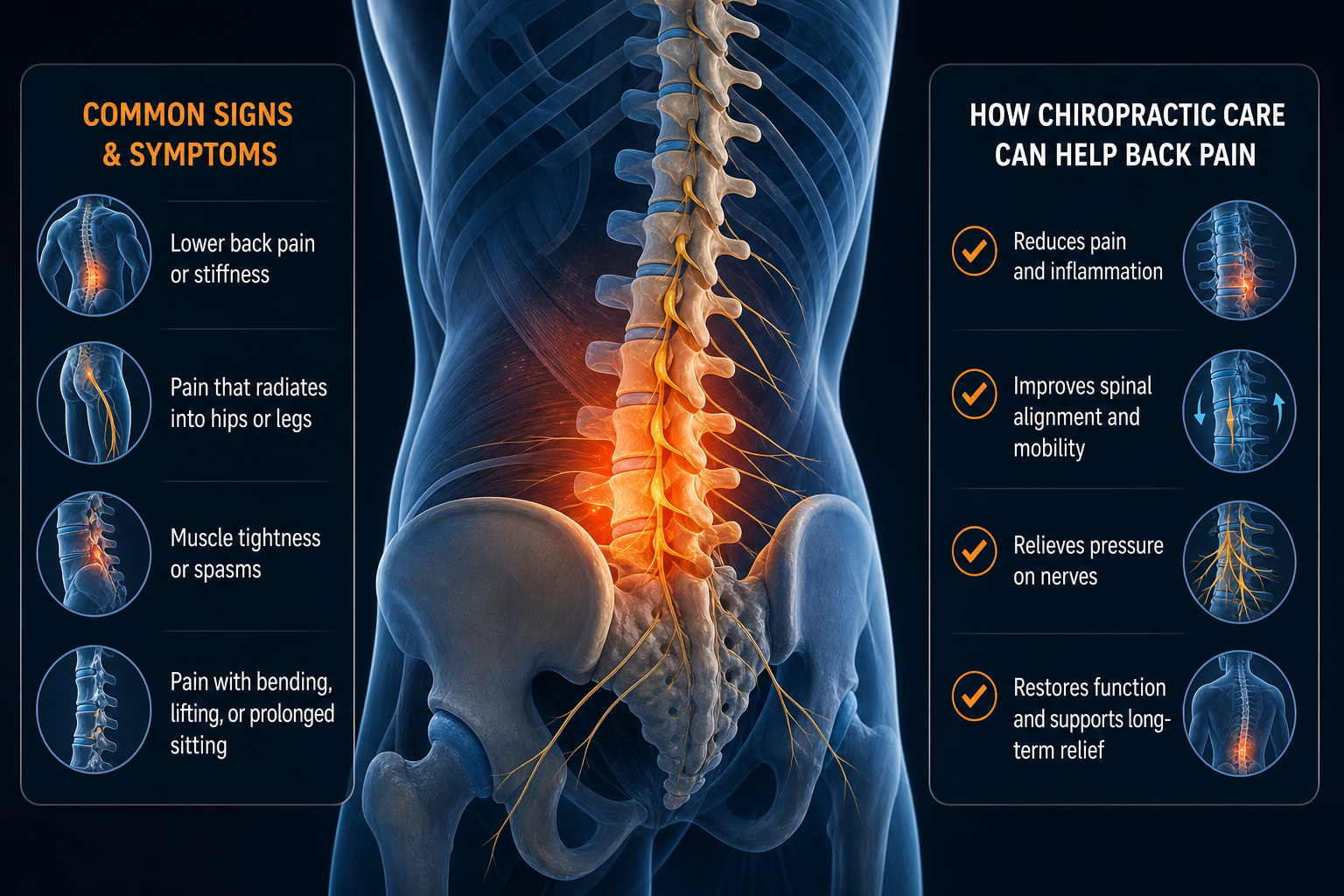
What are the common symptoms of inflammatory spondylopathy?
The most common symptoms of inflammatory spondylopathy are morning stiffness, low back or buttock pain, reduced spinal mobility, and symptoms that improve with activity. Pain often starts deep near one or both sacroiliac joints and may alternate sides. Some people also develop upper back stiffness, neck restriction, or pain around tendon attachment sites.
- Stiff lower back in morning lasting 30 minutes or longer
- Deep ache in the buttock or posterior pelvis
- Symptoms that wake you late at night or early morning
- Loss of lumbar flexion, extension, or rotation
- Hip stiffness, especially after sitting
- Flare-ups after inactivity rather than after exercise alone
Symptoms outside the low back
Inflammatory conditions can also affect areas away from the spine. You may notice heel pain at the Achilles tendon insertion, chest wall tightness around the costovertebral joints, or discomfort where the plantar fascia meets the heel. These findings do not confirm a diagnosis, but they change the evaluation.
Timelines matter. Mechanical strain often settles in 2-4 weeks with activity modification. Inflammatory patterns more often persist beyond 12 weeks, fluctuate, and return quickly when you stop moving.
If back stiffness improves with exercise but returns after prolonged sitting, that pattern is more consistent with inflammation than a simple muscular strain.
If your symptoms also include head and neck tension from guarded posture, you may benefit from learning how spinal mechanics contribute to related issues such as tension headaches and conservative care.
What causes inflammatory spondylopathy and which conditions are linked to it?
The causes of inflammatory spondylopathy are not limited to one trigger. Genetics, immune system activity, gut-related inflammation, and associated inflammatory disorders can all contribute. Providers usually look for a pattern rather than a single event.
Conditions linked to inflammatory back pain
- Ankylosing spondylitis
- Axial spondyloarthritis
- Psoriatic arthritis
- Reactive arthritis
- Inflammatory bowel disease-associated joint involvement
These are some of the main conditions linked to inflammatory back pain. A family history of inflammatory arthritis, psoriasis, bowel inflammation, or recurring tendon insertion pain can raise suspicion. So can pain that starts before age 45 and continues for months.
Inflammation changes how joints move. When the sacroiliac joints stiffen, nearby tissues compensate. The piriformis, quadratus lumborum, and iliopsoas often become overactive. That secondary tension can make the pain feel muscular even when the underlying driver is inflammatory.
Do not self-diagnose from a checklist alone. Similar symptoms can show up with disc irritation, hip joint restriction, or persistent mechanical overload. If you also have leg pain below the knee, numbness, or tingling, compare those features with common sciatica patterns before assuming the source is inflammatory.
How is inflammatory spondylopathy diagnosed?
How is inflammatory spondylopathy diagnosed usually starts with a history and physical exam, not with one single test. A provider looks at symptom timing, spinal mobility, posture, gait, joint tenderness, and whether your pain improves with repeated movement. They may also coordinate imaging or lab work through the appropriate medical channel if your pattern suggests a systemic inflammatory condition.
What a provider may assess at the first visit
- History: onset, morning stiffness duration, night pain, family history, bowel or skin symptoms, and activity response
- ROM testing: lumbar flexion, extension, side-bending, thoracic rotation, and hip mobility
- Palpation: sacroiliac tenderness, paraspinal tone, gluteal trigger points, and chest wall restriction
- Functional tests: squat, sit-to-stand, gait, single-leg balance, and hip hinge mechanics
- Screening for red flags: fever, unexplained weight loss, bowel or bladder changes, progressive weakness
A rehab-focused provider may also check breathing mechanics because limited rib mobility can increase thoracic stiffness. Chiropractors, physical therapists, rehab specialists, and acupuncture providers each evaluate different pieces of the puzzle, but all should be looking for consistent movement patterns and red flags.
If balance symptoms or cervicogenic complaints are part of the picture, Medximity also has patient education on vestibular disorders treatment and vertigo and chiropractic care that explains how a provider separates spinal findings from other causes.
Conservative treatment options for inflammatory spondylopathy
Treatment for inflammatory spondylopathy pain usually centers on preserving mobility, reducing joint stress, improving posture and load tolerance, and keeping surrounding tissues from becoming chronically tight. Natural treatment for inflammatory back pain does not mean ignoring a medical workup when needed. It means using non-invasive care to improve function while the condition is being appropriately evaluated and monitored.
Treatment Primary Goal Expected Outcome Typical Timeline Physical therapy Improve ROM, hip-spine mechanics, endurance Better movement tolerance and less morning stiffness Typically 6-8 visits over 4-6 weeks Chiropractic care Address joint restriction and movement quality Improved segmental mobility in selected patients Often 4-8 visits with reassessment every 2-3 weeks Exercise therapy Maintain spinal extension, thoracic rotation, hip mobility Reduced stiffness flare-ups Daily home program, changes often noticed in 2-3 weeks Massage or soft tissue work Reduce secondary muscle guarding Short-term relief and easier movement 1-2 sessions weekly during flare periods Acupuncture Support pain modulation and muscle relaxation Symptom relief in some patients Commonly 4-6 sessions before reassessment- Physical therapy: often focuses on thoracic extension, hip extension, gluteal strength, and gait mechanics.
- Chiropractic care: may help selected patients with restricted spinal or sacroiliac motion, especially when paired with exercise.
- Exercise therapy: usually produces the most durable change because mobility returns only if you keep moving.
- Acupuncture and massage: can reduce protective muscle tone around the lumbar paraspinals and gluteals.
For related neuromusculoskeletal education, you can also review trigeminal neuralgia treatment with chiropractic and post-concussion natural treatment approaches to see how conservative providers assess complex symptom patterns without defaulting to one explanation.
Daily habits that may support comfort and mobility
Exercises for inflammatory back stiffness work best when done consistently, not aggressively. Your goal is to restore motion in the spine and hips without provoking a prolonged flare. Start with 8-12 minutes each morning.
Simple morning mobility sequence
- Diaphragmatic breathing, 1 minute: lie on your back with knees bent, inhale through the nose, expand the lower ribs, exhale slowly.
- Pelvic tilts, 10 reps: flatten the low back gently into the floor, then release to neutral.
- Cat-camel, 8 reps: move the lumbar and thoracic spine through flexion and extension without forcing end range.
- Prone press-ups, 8-10 reps: lie face down, press onto forearms or hands, keeping hips on the floor if tolerated.
- Half-kneeling hip flexor stretch, 30 seconds each side: squeeze the glute of the kneeling side to target the iliopsoas.
- Thoracic rotation, 6 reps each side: side-lying open-book stretch to improve rib and mid-back mobility.
- Brisk walk, 5-10 minutes: finish with upright walking to reinforce movement.
This routine typically helps within 1-2 weeks if stiffness is movement-responsive. If symptoms spike for more than 24 hours after each session, reduce range and repetitions.
- Avoid sitting longer than 30-45 minutes without standing up.
- Use a small lumbar roll during desk work if slumped posture increases pain.
- Alternate walking, standing, and seated tasks throughout the day.
- Prioritize hip extension and thoracic rotation work, not only hamstring stretching.
If upper cervical mechanics or postural compensation are contributing to other symptoms, Medximity also covers topics such as Meniere’s recovery with upper cervical treatment.
When should you see a provider for back stiffness?
When should I see a provider for back stiffness has a simple answer: seek evaluation if morning stiffness lasts longer than a few weeks, pain repeatedly improves with activity but returns at rest, or your mobility is steadily declining. Persistent inflammatory-type pain deserves a real exam.
- See a provider routinely if symptoms last more than 2-4 weeks.
- Book sooner if stiffness lasts more than 30-60 minutes every morning.
- Seek prompt evaluation if pain wakes you most nights or alternates between buttocks.
- Seek urgent medical attention if you have fever, unexplained weight loss, new bowel or bladder changes, saddle numbness, or progressive leg weakness.
Those last signs are red flags. They are not typical features of uncomplicated mechanical strain or routine inflammatory stiffness.
If you already know your symptoms are mostly spinal and movement-related, a chiropractor, physical therapist, rehabilitation provider, or acupuncture provider may help with conservative management. If your pattern suggests a systemic inflammatory disorder, coordinated medical evaluation is appropriate alongside rehab.
What to Do Next
Start by matching your symptoms to the right provider. If your main problem is morning stiffness, reduced ROM, and recurrent low back or sacroiliac pain, look for a chiropractor, physical therapist, rehabilitation specialist, or acupuncture provider with experience in spine mobility and persistent back pain. Use Medximity to find a chiropractor near you, browse providers, or explore more health topics.
At the first visit, expect questions about timing, stiffness duration, night pain, activity response, family history, and movement limits. Expect ROM testing of the lumbar spine, thoracic spine, hips, and sacroiliac region. Expect a plan that includes home exercises, posture changes, and a short reassessment timeline, commonly 2-3 weeks.
- Routine care: stiffness lasting weeks, reduced flexibility, recurring buttock or low back pain, pain eased by movement
- Prompt care: worsening mobility, repeated night pain, symptoms spreading to other joints or tendon insertions
- Urgent medical care: fever, unexplained weight loss, bowel or bladder changes, saddle numbness, severe or progressive weakness
If you are searching for an inflammatory back pain provider near me, the next step is straightforward: book an evaluation with a qualified conservative provider and get a movement-based plan instead of guessing. Early assessment helps you separate inflammatory patterns from mechanical strain and gives you a practical path to improve comfort and mobility.