Understanding ankylosing spondylitis of the spine: symptoms, causes, and treatment starts with one key fact: this is a chronic inflammatory condition that commonly affects the sacroiliac joints and spine, causing back stiffness that is often worse in the morning and may improve with movement. If you have persistent low back pain, reduced spinal flexibility, or rib cage tightness that lasts for months, a provider evaluation can help separate ankylosing spondylitis from common mechanical back pain and guide conservative care.
Early recognition matters because untreated inflammation can gradually limit motion in the lumbar spine, thoracic spine, and cervical spine. Conservative management often includes targeted physical therapy, mobility work, posture training, breathing exercises, and activity modification designed to maintain function over the long term.
What Is Ankylosing Spondylitis of the Spine?
Ankylosing spondylitis is a form of inflammatory arthritis that most often affects the joints where the spine meets the pelvis. If you are searching “what is ankylosing spondylitis spine,” the plain-language answer is this: it is not ordinary back strain. It is a condition in which ongoing inflammation can stiffen spinal joints and, over time, reduce how well your back and chest move.
The condition usually begins near the sacroiliac joints, then may involve spinal segments, ligaments, and the points where tendons attach to bone. Those attachment points are called entheses. When entheses around the pelvis, ribs, or spine become irritated, you may notice pain with rest, prolonged sitting, or first movement in the morning.
What makes it different from a simple strain
- A strain often starts after lifting, twisting, or overuse.
- Ankylosing spondylitis often develops gradually over weeks to months.
- A strain typically eases with rest for a short period.
- Ankylosing spondylitis commonly produces stiffness after rest and loosens somewhat with movement.
Research commonly cited in rheumatology literature shows ankylosing spondylitis often begins before age 45 and may take years to identify when early symptoms are mistaken for general back pain.
This distinction is why chronic stiffness should not be written off as “just tight muscles.” If your pattern fits inflammatory back pain, a provider may coordinate imaging, mobility testing, and rehabilitation rather than treating it like a short-term flare of mechanical low back pain.
How does ankylosing spondylitis differ from general low back pain?
Ankylosing spondylitis vs low back pain comes down to pattern, timing, and response to activity. Mechanical low back pain usually tracks with tissue overload in muscles, discs, or joints. Ankylosing spondylitis has a more inflammatory pattern: morning stiffness, improvement with gentle activity, and symptoms that persist for longer than 3 months.
Feature Ankylosing Spondylitis General Mechanical Low Back Pain Onset Gradual, often over months Often linked to lifting, bending, or a specific episode Morning stiffness Common, often 30-60+ minutes Usually brief or absent Effect of movement Often improves with movement May worsen with repeated loading Night symptoms Can wake you in the second half of the night Less characteristic Areas involved Sacroiliac joints, spine, rib cage, hips Muscles, discs, facet joints, ligaments Typical recovery Long-term management condition Often improves in 2-6 weeks with conservative careA mechanical flare from lifting may settle within 2 to 6 weeks. Ankylosing spondylitis does not follow that timeline. Instead, you may have recurrent stiffness for months or years, with periods that are better and worse.
If your symptoms also include leg pain, numbness, or burning below the knee, the issue may overlap with another condition such as sciatica. For a related breakdown, see sciatica treatment and understanding the pain.
What are the early signs of ankylosing spondylitis?
The early signs of ankylosing spondylitis usually include persistent low back or buttock pain, morning back stiffness that improves after moving around, and a gradual loss of flexibility. Pain may alternate from one side of the buttock to the other because the sacroiliac joints sit on both sides of the pelvis.
Common early symptom pattern
- Low back or deep buttock pain lasting more than 3 months
- Stiffness after sleep or sitting
- Symptoms easing after walking, stretching, or a warm shower
- Reduced ability to bend forward or rotate your trunk
- Night pain that improves once you get up and move
You may also notice that your stride shortens because the hips and pelvis feel restricted. The gluteal muscles, hip flexors, and spinal extensor muscles often become secondarily tight as your body guards against stiffness.
Loss of chest expansion is another early clue. When inflammation affects the joints connecting the ribs to the spine or sternum, deep breathing can feel restricted during exercise.
Morning stiffness lasting longer than 30 minutes, especially when it improves with activity, is one of the most useful symptom patterns that separates inflammatory spinal pain from a routine strain.
These signs should prompt a formal assessment rather than self-diagnosis. A provider can compare your spinal ROM, posture, gait, and symptom history to determine whether you need further workup.
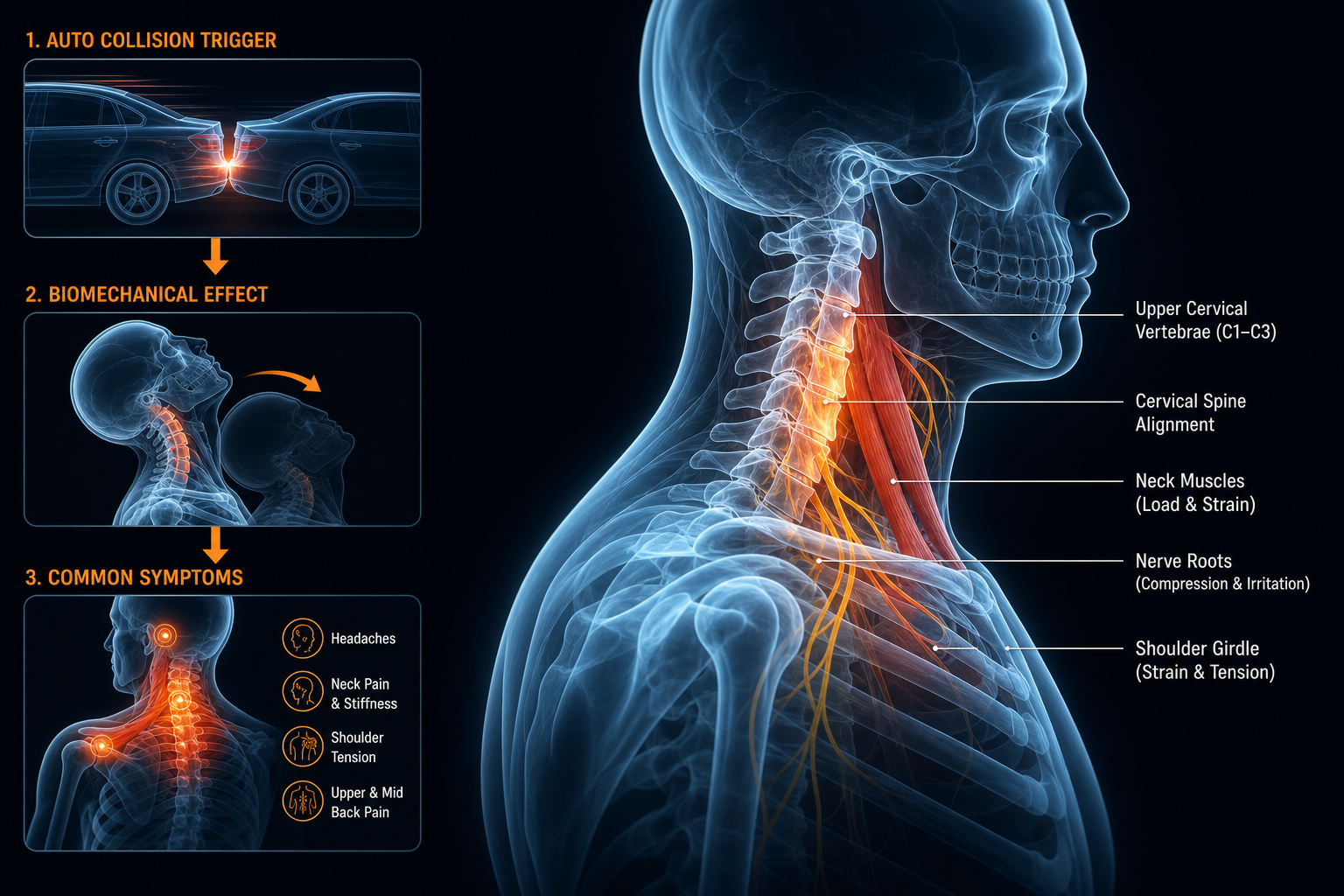
How can ankylosing spondylitis affect more than the low back?
Yes, ankylosing spondylitis can cause hip pain, and it can also affect the mid-back, neck, chest wall, and posture. The condition does not stay neatly isolated to one spot. As stiffness develops, the body compensates upward and downward through connected segments.
Hip involvement matters because the hips help absorb load during walking and standing. If hip extension becomes limited, your lumbar spine and pelvis often move less efficiently, which can magnify stiffness in the low back.
Areas commonly affected outside the low back
- Hips: groin pain, reduced extension, trouble with long strides
- Thoracic spine: stiffness turning or extending the trunk
- Rib cage: reduced chest expansion with deep breaths
- Cervical spine: neck stiffness, difficulty rotating to look over your shoulder
- Shoulder girdle: compensatory tightness from posture changes
Posture changes can develop gradually. A more flexed thoracic posture, forward head position, and reduced lumbar motion are common movement findings. Those patterns can contribute to tension headaches or upper neck strain, which is one reason some patients also benefit from reading about medication free treatment for tension headaches or upper cervical treatment approaches for balance-related symptoms when neck mechanics are part of the broader picture.
Not every patient will develop the same distribution of symptoms.
That is why a full spine and pelvic exam matters more than focusing only on the exact spot that hurts today.
What causes ankylosing spondylitis flare ups and who is at risk?
Possible causes and risk factors include genetic predisposition, immune system activity, and mechanical stress layered on top of inflammation. The exact cause is not fully settled, but providers often look at family history, age at onset, symptom timing, and associated joint or tendon symptoms.
- Family history of inflammatory spinal conditions
- Symptoms beginning before age 45
- Persistent pain with rest rather than only after heavy activity
- Recurring stiffness after sleep or prolonged sitting
- Flares during periods of reduced movement or poor sleep quality
If you are asking what causes ankylosing spondylitis flare ups, common triggers include prolonged inactivity, missed exercise, sustained slumped posture, abrupt training spikes, and inadequate recovery between demanding physical days. These factors do not create the disease by themselves, but they can amplify stiffness and pain in tissues that are already prone to inflammation.
Mechanical overload can still coexist. For example, if you sit in lumbar flexion for 8 to 10 hours daily, the thoracolumbar fascia, hip capsule, and posterior chain muscles may become less tolerant, making an inflammatory pattern feel worse.
Clinical management works best when inflammatory drivers and mechanical contributors are addressed together: movement quality, posture, mobility, workload, sleep position, and regular exercise all matter.
How do providers evaluate ankylosing spondylitis?
How do doctors diagnose ankylosing spondylitis is a common question, and the answer is that diagnosis usually combines history, physical examination, imaging, and sometimes lab work ordered by the appropriate medical provider. No single stretch test confirms it.
Your evaluation typically starts with symptom pattern. A provider will ask how long pain has lasted, whether stiffness is worse in the morning, whether movement helps, and whether the pain wakes you at night. Then they will check posture, spinal motion, rib expansion, gait, and hip mobility.
What a conservative musculoskeletal exam may include
- Observation of standing posture and spinal curves
- ROM testing for lumbar flexion, extension, side-bending, and thoracic rotation
- Hip mobility assessment, especially extension and internal rotation
- Palpation around the sacroiliac joints and surrounding soft tissue
- Functional tests such as walking, sit-to-stand, and deep breathing expansion
Imaging may include X-ray or MRI depending on the stage of the condition and what the referring provider needs to clarify. MRI can show earlier inflammatory changes than X-ray in some cases. Rehabilitation providers then use those findings to shape exercise intensity, posture correction, and mobility goals.
This evaluation should not be used for self-diagnosis. It is a roadmap for deciding whether your pain behaves like inflammatory spinal disease, mechanical low back pain, or a mixed presentation.
If dizziness, neck pain, or vestibular symptoms overlap with your posture pattern, related rehabilitation content may also help, including vestibular disorders treatment and vertigo solutions with chiropractic treatment.
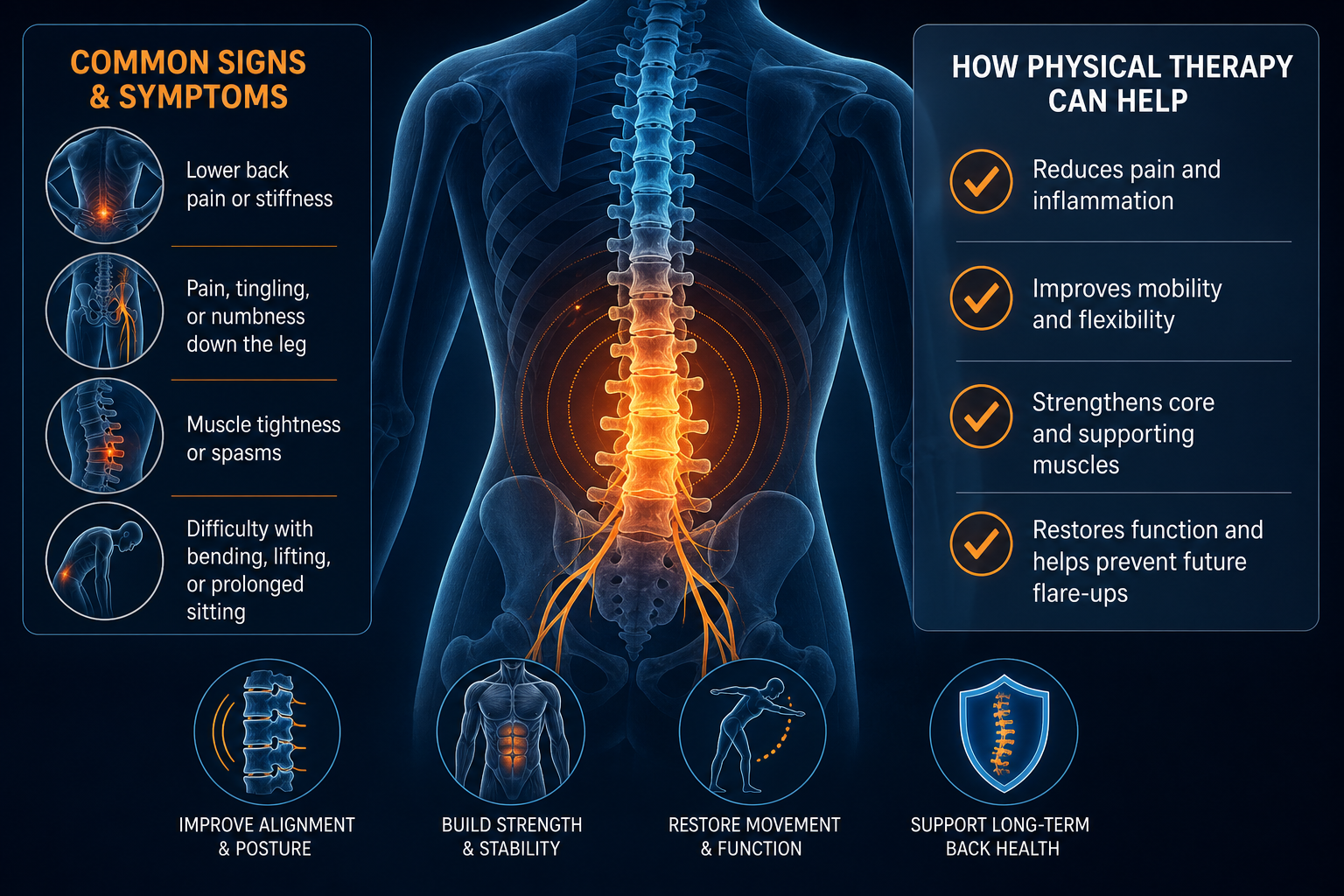
What conservative treatment options help ankylosing spondylitis of the spine?
Non surgical treatment for ankylosing spondylitis focuses on preserving mobility, improving posture, reducing stiffness, and keeping you active. Conservative care does not “cure” the condition, but it can improve function and help you maintain spinal movement over time.
Treatment Primary Goal Expected Outcome Typical Timeline Physical therapy Improve ROM, posture, gait, and strength Better mobility and activity tolerance Typically 6-12 visits over 6-8 weeks, then home program Exercise therapy Maintain spinal extension, hip mobility, chest expansion Less stiffness with daily movement Daily or near-daily, benefits often noticed in 2-4 weeks Manual therapy Address soft-tissue restriction and joint stiffness in selected areas Short-term motion gains and easier movement Often paired with exercise from visit 1 Posture training Reduce flexed posture and improve alignment habits Better standing tolerance and breathing mechanics Usually practiced daily for months Breathing and rib mobility drills Support chest wall mobility Improved deep-breath comfort during activity Often 2-6 weeks for measurable changePhysical therapy programs commonly target the hip flexors, thoracic extensors, gluteus medius, and deep trunk stabilizers. Treatment may include extension-biased mobility work, thoracic rotation drills, gait retraining, and progressive strengthening.
- PT is useful when stiffness limits daily function or posture.
- Chiropractic or manual therapy may help selected joints move more comfortably when paired with exercise.
- Massage can reduce protective muscle tone around the paraspinals and glutes.
- Acupuncture may be included for some patients as part of a broader conservative plan.
Expect management, not a one-visit fix. Most people do best when in-office care transitions to a durable home routine.
What daily habits and home exercises support mobility and posture?
The best exercises for ankylosing spondylitis posture are the ones you can do consistently with good form. Daily mobility work is usually more effective than doing a long session once a week. The goal is to restore extension, preserve hip mobility, and keep the rib cage moving.
Simple home routine: 10 to 15 minutes
- Prone press-up: Lie on your stomach with hands under shoulders. Press your chest up while hips stay down. Move only into mild stretch, not sharp pain. Perform 8 to 10 reps.
- Thoracic extension over a rolled towel: Place a towel roll across the mid-back, support your head, and gently extend over it. Hold 20 to 30 seconds for 3 to 4 reps.
- Half-kneeling hip flexor stretch: Tuck your pelvis slightly and shift forward until you feel stretch in the front of the hip. Hold 30 seconds each side for 2 to 3 rounds.
- Open-book rotation: Lie on your side with knees bent. Rotate the top arm and trunk backward while keeping knees stacked. Do 8 reps each side.
- Diaphragmatic breathing with lateral rib expansion: In sitting or lying, inhale through the nose and direct air into the lower rib cage. Take 5 slow breaths, 2 to 3 sets.
Walk daily if possible. Even 15 to 20 minutes of brisk walking can reduce stiffness after prolonged sitting. Set a timer to stand every 30 to 45 minutes if you work at a desk.
Posture habits also count:
- Raise screens to eye level.
- Use a chair that supports neutral pelvis position.
- Avoid spending hours in deep lumbar flexion.
- Alternate sitting, standing, and walking through the day.
Patients working through broader neurologic or balance-related rehab often use similar consistency principles, which you can see in treating post-concussion syndrome by natural means.
What questions should you ask a provider during an evaluation?
Questions to ask about ankylosing spondylitis should help you understand diagnosis, movement limits, and your home plan. Good questions produce a practical care roadmap, not vague reassurance.
- Does my symptom pattern look inflammatory, mechanical, or mixed?
- Which joints or movement restrictions are most involved right now?
- Do I need imaging such as X-ray or MRI based on my history and exam?
- Which exercises should I do daily, and which should I avoid during a flare?
- What posture changes matter most for work, sleep, and driving?
- How will we measure progress: ROM, walking tolerance, chest expansion, pain frequency?
- When should I be referred to another specialist?
Ask for objective baselines. Examples include fingertip-to-floor distance, hip extension range, thoracic rotation, chest expansion, and walking tolerance. Those measures make it easier to tell whether a program is working over the next 4 to 8 weeks.
If you also have facial pain, upper neck involvement, or atypical nerve symptoms, differentials may need to be considered. Related educational material includes trigeminal neuralgia treatment with chiropractic.
What to Do Next
If your back pain has lasted longer than 3 months, is worst in the morning, improves with movement, or includes buttock, hip, rib cage, or neck stiffness, schedule an evaluation with a provider experienced in spine rehabilitation. Good starting points include a physical therapist, rehabilitation-focused chiropractic provider, or another spine specialist who can coordinate imaging and further workup when needed.
At your first visit, expect a review of symptom timing, posture, spinal ROM, hip motion, gait, and functional limits. Bring a short history of when symptoms started, what makes them better or worse, and whether night pain or prolonged morning stiffness is present.
- Seek routine care soon if stiffness is recurring, posture is changing, or activity tolerance is dropping.
- Seek urgent medical care if you develop sudden severe weakness, loss of bowel or bladder control, major trauma, unexplained fever with severe spinal pain, or chest pain and shortness of breath that are new or worsening.
You do not need to guess whether this is ordinary back pain. You need a structured exam.
To get started, find a physical therapy provider near you, find a chiropractic provider near you, browse providers, or explore more health topics on Medximity.
Frequently Asked Questions
How long does ankylosing spondylitis last?
Ankylosing spondylitis is usually a long-term condition rather than a short episode. Symptoms may fluctuate, but the condition often requires ongoing management focused on mobility, posture, and function. A mechanical back strain may improve in 2 to 6 weeks, while ankylosing spondylitis commonly needs long-range exercise and monitoring.
Can ankylosing spondylitis cause hip pain?
Yes. Hip involvement is common and may cause groin pain, reduced stride length, and difficulty extending the leg behind you. Restricted hip motion often makes low back stiffness worse because the pelvis and lumbar spine must compensate.
What does morning stiffness that improves usually mean?
Morning back stiffness that improves with movement is a classic inflammatory pattern. It does not confirm ankylosing spondylitis by itself, but it is one of the main reasons providers investigate inflammatory spinal conditions rather than treating the problem as a simple strain.
Can exercise make ankylosing spondylitis worse?
Wrong exercise dose can aggravate symptoms, but well-chosen movement usually helps. Daily mobility, walking, posture drills, and progressive strengthening are standard conservative tools. Long periods of inactivity often make stiffness worse.
Should you still get checked if the pain comes and goes?
Yes. Ankylosing spondylitis can be intermittent early on. Recurrent bouts of buttock pain, low back stiffness, or rib cage tightness over months deserve evaluation even if you have good days between flares.
What type of provider should you see?
Start with a provider who evaluates spine function and can recognize inflammatory patterns, such as a physical therapist, rehabilitation-focused chiropractic provider, or another musculoskeletal specialist. If your history suggests inflammatory arthritis, they may coordinate further medical evaluation and imaging.