Understanding osteoporosis-related left shoulder fractures: symptoms, causes, and treatment starts with one key fact: a weakened bone can break near the shoulder after a low-force fall, bump, or sudden brace with the arm. Most osteoporosis-related shoulder fractures involve the proximal humerus, and early care focuses on confirming the break, protecting the bone, restoring motion safely, and reducing fall risk during recovery.
If you have pain when lifting your arm after a fall, swelling, bruising, or sharp pain around the top of the left arm, get the shoulder checked promptly. Mild soreness from a strain usually improves over a few days; a fracture often causes persistent pain, marked loss of motion, and tenderness directly over bone.
What Is an Osteoporosis-Related Left Shoulder Fracture?
An osteoporosis-related left shoulder fracture is a break in bone near the left shoulder caused or made more likely by low bone density. The most common site is the proximal humerus, the upper end of the arm bone that forms part of the shoulder joint with the scapula. Less often, the fracture may involve the clavicle or the shoulder blade.
If you are asking what is an osteoporosis shoulder fracture, the short answer is this: bone has become porous enough that a low-energy event can cause a crack or complete break. That event may be a simple trip, a fall onto an outstretched hand, or a direct hit to the side of the shoulder.
- Most common location: proximal humerus
- Usual mechanism: fall onto the side, elbow, or hand
- Typical age pattern: more common in older adults, especially after midlife bone loss
- Main problem: pain plus sudden loss of usable shoulder motion
Research consistently places proximal humerus fractures among the more common fragility fractures in older adults, behind hip and wrist fractures. That matters because even a “small” shoulder fracture can sharply reduce your ability to dress, reach, sleep comfortably, or use the arm for support.
Bone quality changes the injury threshold. A younger person may bruise the shoulder in a fall that causes a fracture in osteoporotic bone.
Why Does Osteoporosis Make Shoulder Fractures More Likely?
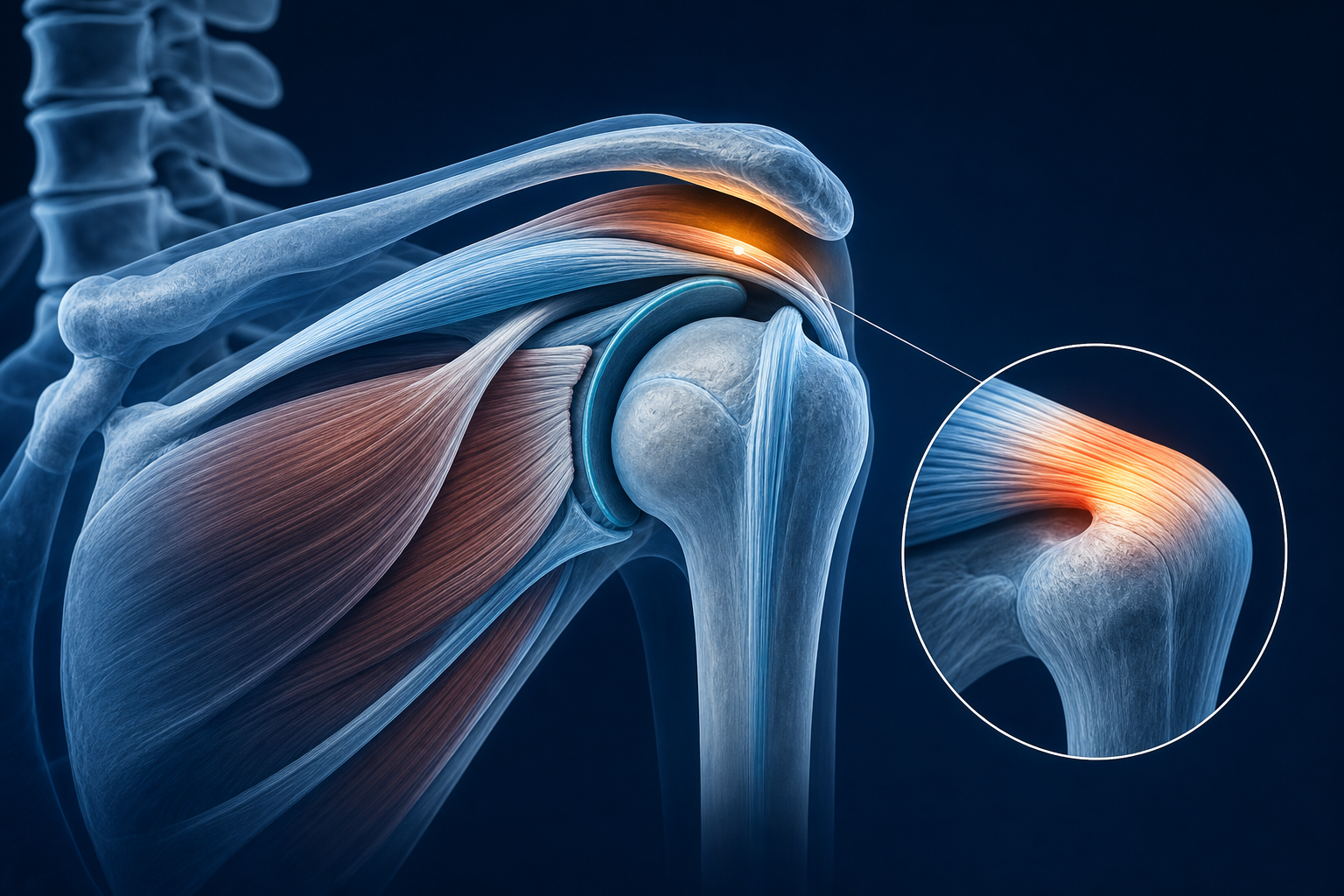
Osteoporosis makes shoulder fractures more likely because it thins the internal bone structure and reduces the bone’s ability to absorb force. The outer shell becomes less resilient, and the inner trabecular bone loses density. In the proximal humerus, that means a minor impact can create enough stress to break the bone near the humeral head or surgical neck.
Why osteoporosis causes shoulder fractures
The shoulder is not a weight-bearing joint like the hip, but it still takes force during a fall. When you reach out to catch yourself, load travels from the hand and forearm into the humerus. If you land directly on the shoulder, the force goes straight into the upper arm bone and glenohumeral joint region.
- Lower bone mineral density means less force is needed to create a fracture.
- Age-related balance changes increase fall frequency.
- Reduced muscle mass lowers your ability to absorb impact.
- Poor reaction speed makes sideways and forward falls more dangerous.
Fragility fractures commonly happen after a standing-height fall, not a major crash. That low-force mechanism is a major clue that underlying bone weakness may be present.
Fall risk and bone health often overlap. If you also have dizziness or balance problems, that raises the chance of another injury. Supportive care for balance issues may matter during recovery, and you can learn more about vestibular disorders treatment if unsteadiness is part of the problem.
What Are the Common Symptoms of a Left Shoulder Fracture?
Left shoulder fracture symptoms in older adults usually include immediate pain, swelling, bruising, and sharp pain with attempted arm motion. The shoulder may look flattened, the upper arm may bruise over 24 to 72 hours, and you may not be able to raise the arm more than a few degrees.
A fracture hurts differently than general soreness. Muscle soreness tends to ease with gentle use. A fracture often produces focal bony tenderness and pain with even small movements such as rolling in bed or reaching for a cup.
Signs that suggest fracture rather than a strain
- Pain when lifting arm after fall that does not improve after rest
- Tenderness over the upper humerus, not just the deltoid muscle
- Visible swelling or bruising down the upper arm
- Sudden weakness or inability to use the arm normally
- Pain with gentle rotation of the shoulder
Red flags that need urgent evaluation
- Obvious deformity
- Numbness in the arm or hand
- Cool, pale, or bluish hand
- Severe swelling that increases quickly
- Shortness of breath, chest pain, or head injury after the fall
What Types of Shoulder Fractures Happen With Osteoporosis?
The main types of shoulder fractures from osteoporosis occur near the top of the humerus. Providers often describe them by location and by whether the broken pieces are displaced.
- Proximal humerus fracture: the most common osteoporosis-related shoulder fracture
- Surgical neck fracture: just below the humeral head
- Greater tuberosity fracture: where the rotator cuff tendons attach
- Lesser tuberosity fracture: less common, but affects internal rotation
- Clavicle fracture: can occur after a direct fall onto the shoulder
The nearby soft tissues matter too. The rotator cuff, deltoid, and axillary nerve can be irritated after injury even when the main problem is the bone. That is one reason shoulder motion often stays limited after the initial pain settles.
Displacement changes treatment. A nondisplaced fracture means the pieces are still aligned. A displaced fracture means the bone fragments have moved enough to change shoulder mechanics and require closer follow-up.
Neck and upper-back posture also influence recovery mechanics. If your shoulder pain is paired with neck tension, mobility work later in rehab may overlap with approaches used in medication free treatment for tension headaches, especially when guarding affects the upper trapezius and cervical muscles.
How Do Providers Evaluate a Suspected Shoulder Fracture?
How do doctors diagnose shoulder fracture is usually straightforward: history, exam, and imaging. The key history is the mechanism of injury, the exact pain location, whether you can move the arm, and whether there is numbness or color change in the hand.
The exam checks the bones, joint position, swelling, circulation, and nerve function. Providers often test light touch over the outer shoulder because that area reflects axillary nerve function.
- Ask how you fell and when the pain started.
- Examine the shoulder, upper arm, elbow, and collarbone.
- Check pulses, hand warmth, and finger movement.
- Order X-ray views of the shoulder and humerus.
- Use additional imaging if the fracture pattern is unclear.
X-ray is the usual first test. It shows alignment, displacement, and fracture location. If pain is severe but X-ray is unclear, more detailed imaging may be used to look at the humeral head, tuberosities, or joint surface.
If the fall also caused dizziness, balance trouble, or head symptoms, that needs separate attention. Medximity has more education on vertigo solution with chiropractic treatment and treating post-concussion syndrome by natural means when those issues affect recovery planning.
Conservative Treatment Support and Early Care
Shoulder fracture treatment without surgery is common for stable or nondisplaced fractures, especially proximal humerus injuries that remain aligned. Early care aims to protect the bone, control swelling, maintain circulation, and prevent shoulder stiffness from becoming the next problem.
The first phase usually lasts about 1 to 3 weeks, depending on fracture pattern and pain level. During that window, the arm is commonly supported in a sling, but total stillness is not the goal. Too much immobilization can stiffen the shoulder, elbow, wrist, and hand.
What early conservative care usually includes
- Sling support as directed by your provider
- Frequent hand, wrist, and elbow motion
- Sleep positioning with pillows behind the trunk and under the arm
- Guided posture correction to avoid rounded-shoulder guarding
- Activity modification: no lifting, pushing, pulling, or overhead reach until cleared
Manual therapy and gentle bodywork may later help nearby muscle guarding, but they should not stress the healing fracture site. Recovery works best when the plan follows imaging and the provider’s movement precautions.
How Does Physical Therapy After Shoulder Fracture Help?
Physical therapy after shoulder fracture helps you regain ROM, scapular control, and arm function without overloading healing bone. The timeline depends on fracture stability, age, baseline bone health, and whether the rotator cuff or joint capsule has become stiff.
If you are asking how long does shoulder fracture heal, bone healing often takes about 6 to 8 weeks for early union, while useful function may continue improving for 3 to 6 months. Some stiffness, especially in overhead reach and external rotation, can take longer.
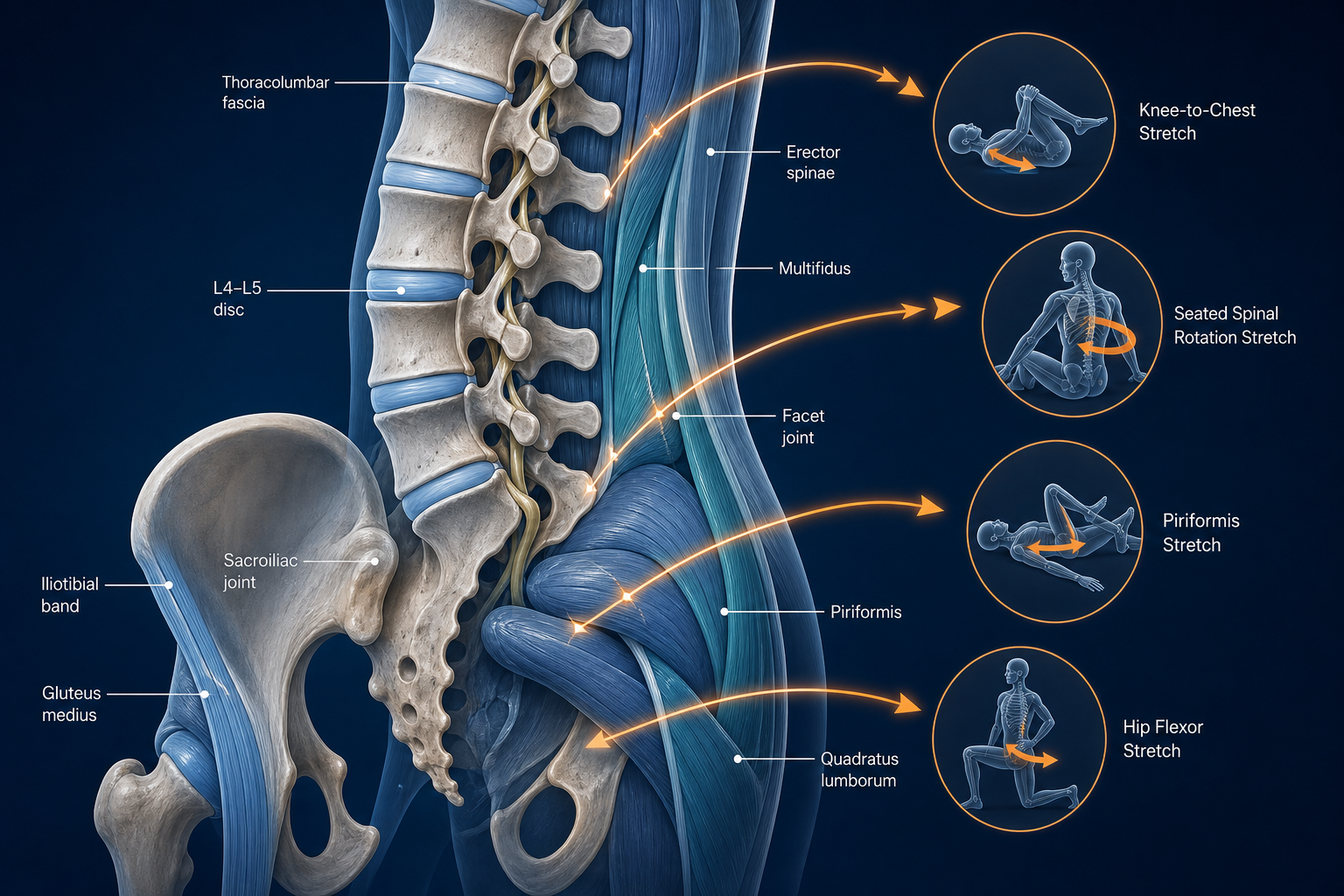
Typical rehab sequence
- Protected motion: pendulum work, hand pumps, elbow bends, posture drills
- Assisted ROM: table slides, cane-assisted flexion, gentle external rotation
- Active ROM: lifting the arm under control without shrugging
- Strengthening: rotator cuff, scapular stabilizers, and deltoid work
One safe home protocol often used after clearance is the pendulum exercise:
- Lean forward with your uninjured hand supported on a table.
- Let the injured arm hang relaxed.
- Move your body to create small circles, front-back swings, then side-to-side motion.
- Keep the shoulder relaxed. Do not actively lift the arm.
- Perform 20 to 30 seconds in each direction, 2 to 3 times daily, only if cleared by your provider.
That drill protects the shoulder from full stiffness while keeping force low across the proximal humerus.
If altered posture during recovery starts causing neck or nerve symptoms farther down the arm, related rehab concepts may overlap with education on sciatica treatment and understanding the pain, where movement quality and nerve-friendly loading also matter.
What Daily Activities Become Harder During Recovery, and How Can You Adapt?
Daily tasks hard with shoulder fracture usually include dressing, bathing, bed mobility, reaching shelves, carrying groceries, and using the arm to push up from a chair. The biggest mistake is trying to “test” the shoulder too early.
- Wear front-button or zip-front clothing.
- Dress the injured arm first; undress it last.
- Keep dishes, toiletries, and clothes between waist and chest height.
- Use two pillows or a reclined position for sleep.
- Avoid lifting more than your provider allows, even if pain drops quickly.
Sleeping is often worst during the first 2 to 4 weeks. A semi-reclined position usually places less pull on the shoulder than lying flat. Reaching behind your back commonly returns later than forward motion because the capsule and rotator cuff tighten quickly.
Caregivers should watch transfers, bathroom setup, throw rugs, and poor lighting. If balance is limited, reduce unnecessary walking while carrying objects. Falls during the first month can turn a stable fracture into a more complex one.
The goal during recovery is not rest alone. The goal is protected movement: enough motion to prevent stiffness, not enough force to disturb healing.
Bone Health, Fall Prevention, and Long-Term Recovery
How to prevent falls after fracture starts at home. Bone healing solves the current injury; fall prevention helps prevent the next one. Osteoporosis-related fractures often come in clusters if balance, strength, vision, footwear, and home layout stay unchanged.
- Remove loose rugs and cords from walking paths.
- Use night lights from bed to bathroom.
- Wear low-heel shoes with firm grip.
- Keep frequently used items at easy reach height.
- Start lower-extremity balance and strength training when cleared.
Posture matters here too. Thoracic rounding shifts your center of mass forward and can make trips harder to correct. Rehab often includes scapular retraction work, thoracic extension drills, and gait practice.
If dizziness contributes to falls, address it directly rather than blaming the fracture alone. Related education on Meniere’s recovery with upper cervical treatment may be useful if recurring balance symptoms are part of your history.
Long-term bone support usually includes nutrition review, weight-bearing exercise for the legs, and provider-guided bone health follow-up. Your shoulder healed because it had to. Your skeleton still needs a plan.
What to Do Next
If you suspect a fracture, get prompt evaluation from an urgent care provider, orthopedic provider, or rehabilitation-focused provider who can coordinate imaging and follow-up. If the injury has already been diagnosed and you are entering recovery, a physical therapist and conservative musculoskeletal provider can help restore motion, posture, and safe function.
- Seek urgent care now if you have deformity, severe swelling, numbness, a cold hand, shortness of breath, or head injury after the fall.
- Schedule routine follow-up soon if the fracture is stable but pain, stiffness, or daily function are limiting recovery.
- At your first rehab visit, expect ROM testing, posture assessment, movement precautions, and a stepwise home program.
- Bring your imaging report, sling instructions, and a list of tasks you cannot currently do.
If you are searching for a shoulder fracture specialist near me, start here to find a physical therapist near you, browse providers, or explore more health topics. The right next step is not guessing whether it will settle on its own. It is confirming the diagnosis, protecting the bone, and starting guided recovery at the right time.