Understanding Osteoporosis-Related Fractures: Symptoms, Causes, and Treatment starts with one fact: weakened bone can break from a low-force event such as a minor fall, a twist, lifting groceries, or even a cough. The most common sites are the vertebral bodies of the spine, femoral neck of the hip, distal radius of the wrist, ribs, and pelvis. Early evaluation matters because a first fragility fracture often predicts higher risk for another fracture within the next 1-2 years.
What Is an Osteoporosis-Related Fracture?
An osteoporosis-related fracture is a bone break caused by reduced bone density and poor bone microarchitecture, usually after force that would not break healthy bone. Clinicians often call this a fragility fracture.
Bone is living tissue. Osteoblasts build bone, osteoclasts remove old bone, and normal loading from walking, resistance training, and daily movement helps maintain bone strength. Osteoporosis shifts that balance toward bone loss, making the trabecular bone inside the spine, hip, wrist, and ribs less able to absorb load.
About 1 in 3 women and 1 in 5 men over age 50 experience an osteoporosis-related fracture during their lifetime, according to large international osteoporosis estimates.
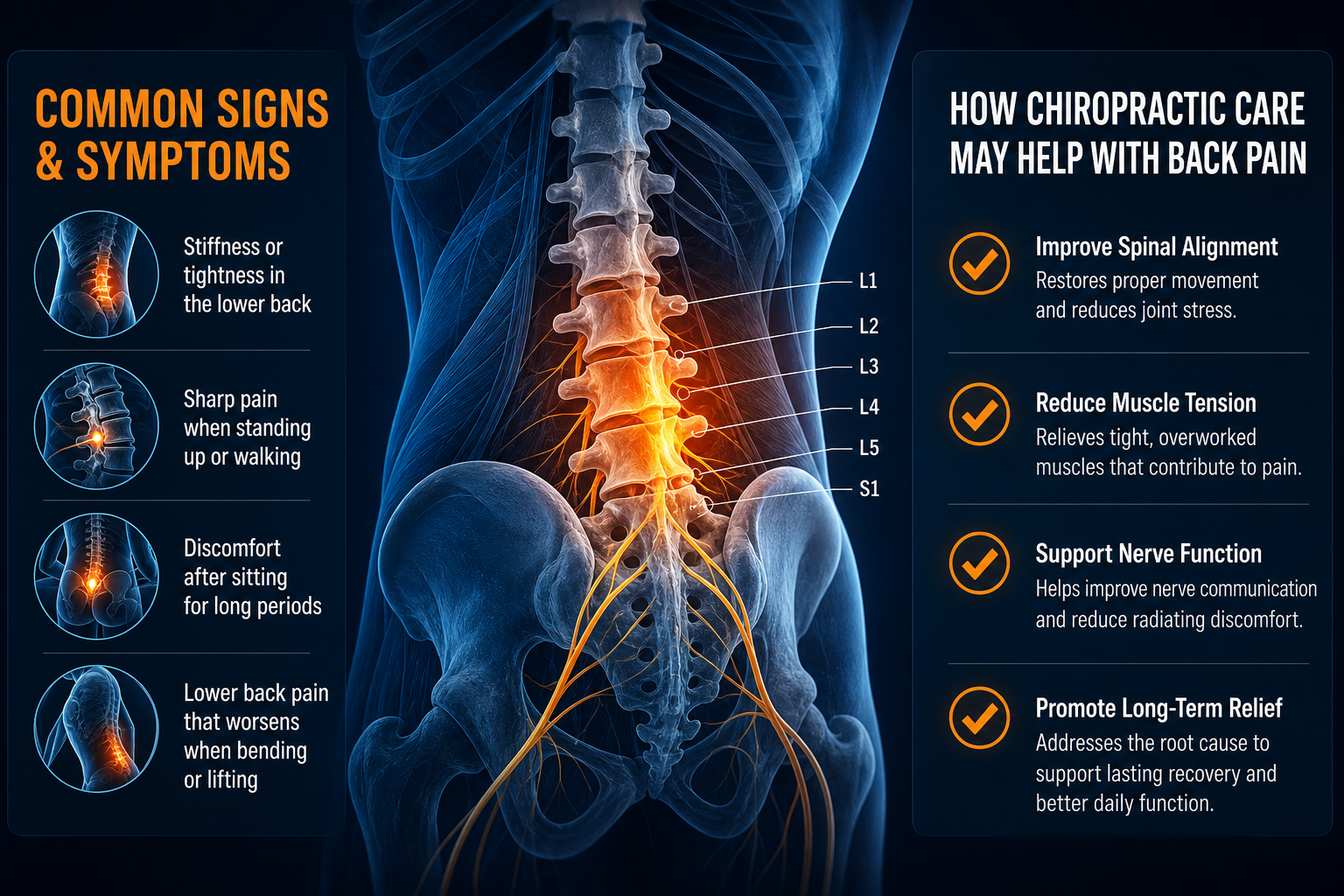
A fracture may occur after a clear fall, but it may also appear after bending, reaching, or lifting. Vertebral compression fractures are especially easy to miss because pain may be mild at first or mistaken for muscle strain in the thoracic or lumbar spine.
- Fragility fracture: a break from standing-height trauma or less.
- Compression fracture: collapse of a spinal vertebral body, often wedge-shaped.
- Kyphosis: forward rounding of the upper back, often linked with multiple thoracic compression fractures.
- Low bone density: reduced mineral content measured most often by DEXA scan.
Osteoporosis does not mean you should stop moving. It means your movement plan should be specific: safer loading, better balance, stronger hips, improved posture, and fall-risk control.
What Does an Osteoporosis Fracture Feel Like?
What does an osteoporosis fracture feel like? The answer depends on the bone involved, but sudden focal pain after a fall, twist, or lift deserves evaluation, especially if you already know you have low bone density.
Common fracture sites and symptoms
Hip fractures often cause groin or outer hip pain and difficulty bearing weight. Wrist fractures usually cause swelling, tenderness, and pain with gripping after landing on an outstretched hand. Rib fractures may cause sharp pain with breathing, coughing, rolling in bed, or pressing over one rib.
Fracture site Typical symptoms Usual recovery timeline Vertebral body Mid-back or low-back pain, height loss, increased kyphosis, pain with standing 6-12 weeks for bone healing; posture and strength work often 12+ weeks Distal radius Wrist swelling, pain with grip, reduced ROM, tenderness near the thumb-side wrist 6-8 weeks for bone healing; grip and wrist ROM often improve over 8-12 weeks Femoral neck or pelvis Groin pain, buttock pain, inability to walk normally, pain with weight bearing Often 8-12+ weeks, depending on fracture type and weight-bearing status Rib Sharp pain with breathing, coughing, twisting, or side-bending 4-8 weeks for many uncomplicated rib fracturesSeek emergency care now for severe pain after a fall, inability to stand or walk, new leg weakness, loss of bladder or bowel control, chest pain, shortness of breath, head injury, or new confusion.
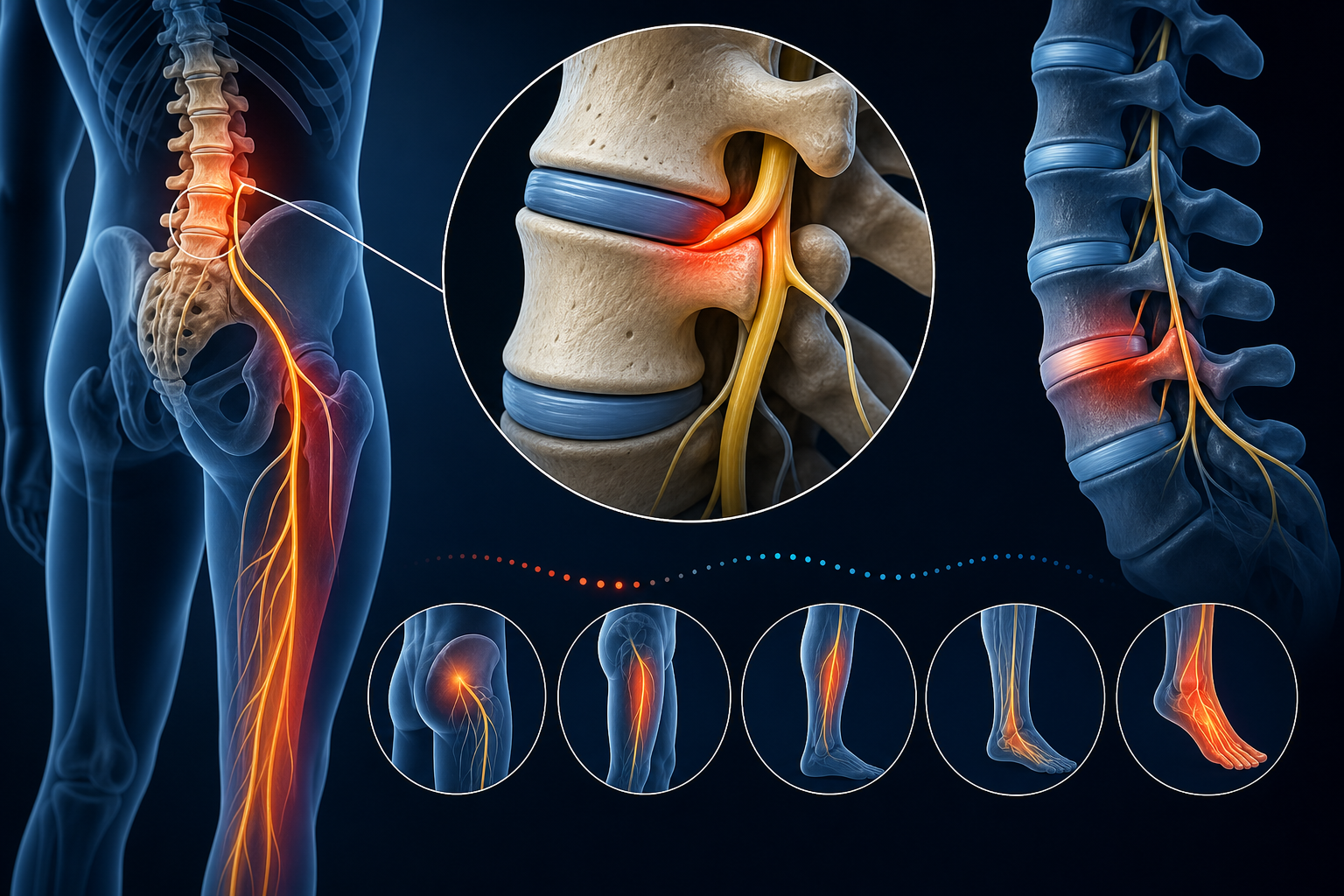
For nerve-like leg pain that travels below the knee, compare symptoms with sciatica pain patterns, but do not assume radiating pain is harmless after a fall.
How Do Vertebral Compression Fractures Become “Silent”?
Vertebral compression fractures can be silent because the vertebral body may collapse gradually instead of breaking with one obvious pain event. Vertebral compression fracture symptoms no pain may still include measurable height loss, a more rounded upper back, reduced spinal extension, and fatigue during standing or walking.
The thoracic spine, especially T7-T12, and the thoracolumbar junction near T12-L1 are common compression sites. The anterior portion of the vertebral body often loses height first, creating a wedge shape. Multiple wedge fractures can increase kyphosis and shift the head and rib cage forward, raising load through the paraspinal muscles, facet joints, and posterior ligaments.
Signs that should prompt imaging discussion
- Loss of height of 1 inch or more from your earlier adult height.
- Sudden back pain after bending, coughing, lifting, or a minor fall.
- New forward rounding of the mid-back.
- Pain that worsens with standing and improves when lying down.
- New tenderness directly over one thoracic or lumbar vertebra.
Plain X-ray can identify many compression fractures. MRI is often used when the provider needs to determine whether the fracture is recent, whether bone swelling is present, or whether the spinal canal or nerve roots are involved.
Dizziness and balance problems increase fall exposure. If unsteadiness is part of your fall history, review vestibular disorder treatment options and ask your provider whether vestibular rehab belongs in your plan.
Is It Acute Fracture Pain or Chronic Osteoporosis Back Pain?
The osteoporosis back pain vs fracture difference usually comes down to timing, location, and mechanical behavior. Acute fracture pain often starts suddenly, feels focal over one bone, and worsens with loading; chronic osteoporosis-related back pain often builds from posture change, muscle fatigue, stiffness, and altered spinal mechanics.
If you ask, “why does my back hurt after a minor fall,” treat the fall as clinically relevant until a provider rules out fracture. Osteoporosis lowers the threshold for injury. A fall that looks small may still overload the sacrum, pelvis, ribs, or vertebral bodies.
Feature Acute fracture pain Chronic osteoporosis-related back pain Onset Sudden after fall, cough, twist, lift, or bend Gradual over weeks to months Location Focal tenderness over one bone or spinal level Broader ache across paraspinals, ribs, or low back Movement pattern Worse with standing, walking, rolling, or spinal flexion Often worse after prolonged posture or deconditioning Next step Clinical exam and possible imaging Posture, strengthening, mobility, and bone-health screeningAvoid repeated loaded spinal flexion when a fracture is suspected. Sit-to-stand training, hip-hinge mechanics, supported walking, and neutral-spine breathing are safer early choices until your provider gives clearance.
For balance-related head and neck symptoms after a fall, post-concussion rehabilitation guidance may help you understand when head trauma needs a separate evaluation.
Who Is at Risk, and How Are DEXA Scans and FRAX Scores Used?
Osteoporosis fracture risk rises when bone density drops and fall risk increases. Age, prior fracture, low body weight, reduced strength, poor vision, low vitamin D status, smoking history, heavy alcohol intake, and family history all matter.
Osteoporosis fracture risk factors in women over 60
Women over 60 have higher fracture risk because bone density often declines faster after menopause. The wrist, vertebral bodies, and hip become higher-risk sites, especially when balance, leg strength, and reaction time decline at the same time.
Can men get osteoporosis related fractures?
Yes. Men get osteoporosis-related fractures, and they are often under-screened. Men with prior low-force fracture, low body weight, long periods of low activity, smoking history, heavy alcohol intake, or chronic inflammatory conditions should ask about bone-density testing.
How is osteoporosis diagnosed DEXA scan explained in plain terms: a DEXA scan estimates bone mineral density at sites such as the lumbar spine and hip. The result includes a T-score. A T-score of -2.5 or lower meets the standard definition of osteoporosis.
- Normal bone density: T-score of -1.0 or above.
- Low bone density: T-score between -1.0 and -2.5.
- Osteoporosis: T-score of -2.5 or lower.
- FRAX score: a 10-year estimate of major osteoporotic fracture and hip fracture risk using clinical risk factors, with or without DEXA data.
FRAX does not replace a physical exam. It helps your provider decide how aggressive prevention should be, including balance training, strengthening, nutrition targets, and referral when risk is high.
Which Conservative Treatment Options Help Osteoporosis-Related Fractures?
Conservative care focuses on protection during early bone healing, then progressive loading to restore ROM, strength, posture, gait, and confidence with daily tasks. Osteoporosis fracture treatment without procedure-based care options may include bracing when appropriate, PT, supervised walking, balance training, low-force manual care, nutrition planning, and home safety changes.
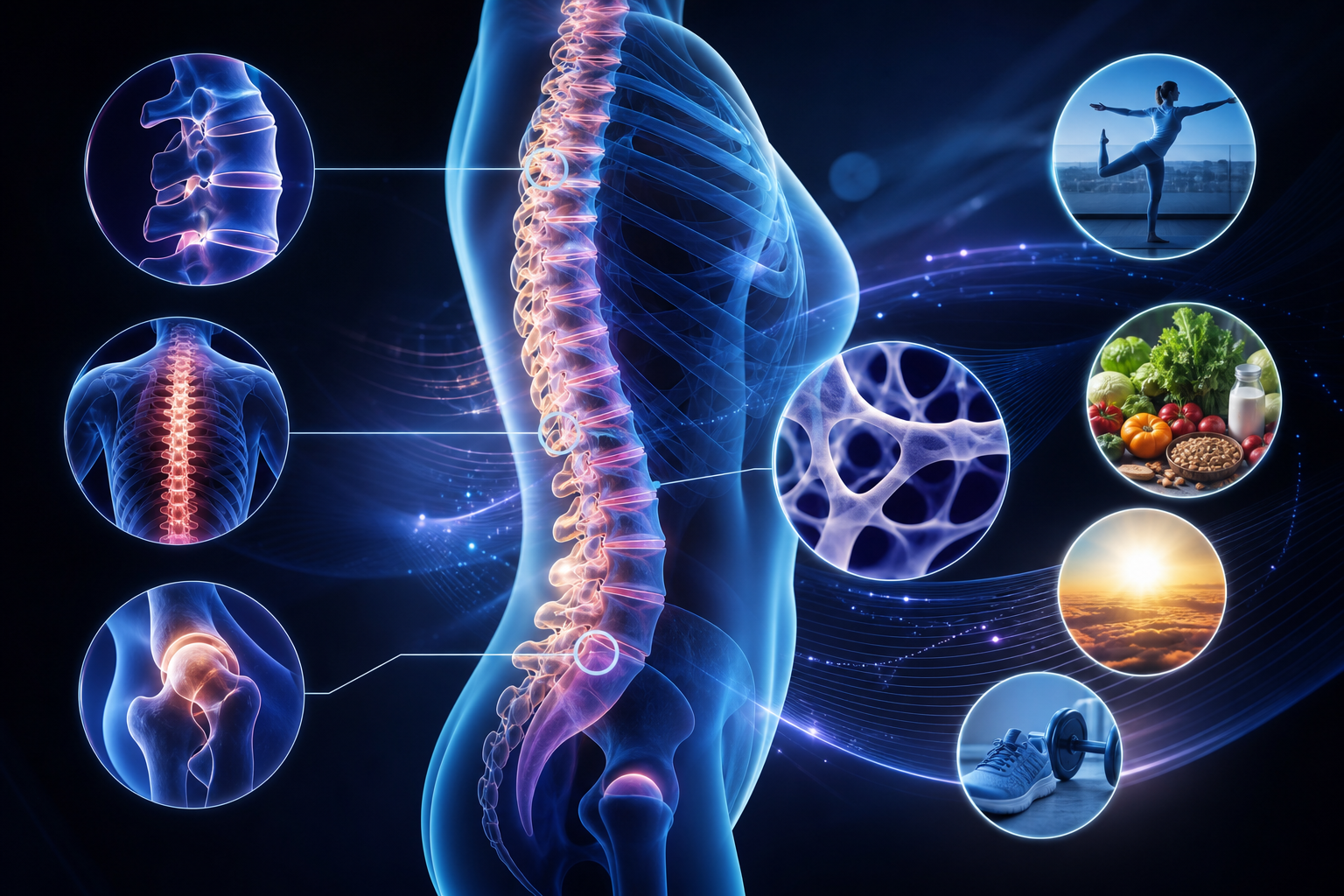
Treatment Expected outcome Typical timeline Activity modification Limits painful loading while bone healing begins First 1-3 weeks, adjusted by symptoms and imaging Physical therapy Improves gait, hip strength, spinal extension tolerance, and safe transfers Typically 6-12 visits over 6-10 weeks Low-force chiropractic care Reduces joint stiffness and improves mechanics without high-force thrusting at fragile areas Often 4-8 visits, then reassessment Balance training Reduces fall risk by improving ankle strategy, hip strategy, and reaction control 8-12 weeks for measurable balance gains Nutrition and loading plan Supports bone remodeling with protein, minerals, vitamin D, vitamin K2, magnesium, and progressive weight-bearing activity Ongoing; reassess strength and habits every 4-6 weeksFoods and vitamins that strengthen bones naturally
Bone health needs more than calcium. Protein supports collagen matrix. Vitamin D supports calcium absorption. Vitamin K2 helps regulate calcium handling in bone tissue. Magnesium supports mineral metabolism and muscle function. Weight-bearing activity tells bone where strength is needed.
- Include protein at each meal from sources that fit your diet.
- Use weight-bearing activity such as walking, step-ups, or sit-to-stands when cleared.
- Train hip abductors, especially the gluteus medius, to reduce fall risk.
- Ask your provider whether lab testing is appropriate before changing supplements.
To compare conservative providers in your area, browse providers and review experience with osteoporosis, rehab, and balance training.
How Can Chiropractic Care, Posture Training, and Fall Prevention Be Adapted Safely?
A chiropractor can treat a patient with osteoporosis safely when care is modified for bone density, fracture history, imaging findings, and current symptoms. High-force thrusting over a known or suspected fracture site is not appropriate; low-force methods, soft-tissue work, positioning support, and rehab-based care are safer choices.
Chiropractic care may focus on the cervical spine, thoracic mobility above and below painful areas, rib mechanics, pelvic alignment, breathing mechanics, and movement coaching. For patients with kyphosis, the goal is not forcing the spine straight; the goal is improving extension tolerance, scapular control, hip strength, and safe daily mechanics.
Balance exercises to prevent falls with osteoporosis
Start balance work near a counter. Stop if pain increases sharply, dizziness appears, or your foot placement becomes unsafe.
- Stand with both hands lightly on a counter and feet hip-width apart.
- Shift weight slowly to the right foot for 5 seconds, keeping the big toe, little toe, and heel grounded.
- Shift to the left foot for 5 seconds.
- Repeat 10 shifts per side.
- Progress by using one hand on the counter, then fingertip support, only if you stay steady.
- Add 2 sets daily for 2 weeks, then ask your PT or chiropractor about tandem stance or step-tap progressions.
Vestibular problems can undermine balance training. If spinning or motion-triggered dizziness occurs, compare symptoms with chiropractic care for vertigo and ask whether vestibular screening is needed.
For upper-cervical and balance-related conditions, upper cervical care for Meniere’s symptoms explains how neck mechanics and balance systems may be assessed in conservative care.
Frequently Asked Questions About Osteoporosis Fractures
What are the first signs of an osteoporosis-related fracture?
The first signs are sudden focal pain after a minor fall, new spinal tenderness, difficulty standing or walking, wrist swelling after landing on the hand, rib pain with breathing, or new height loss. Vertebral fractures may also show up as increased kyphosis rather than severe pain.
How long does a spinal compression fracture take to heal?
A spinal compression fracture typically needs 6-12 weeks for bone healing, but posture, strength, and walking tolerance may need 3-6 months of progressive rehab. Pain should trend downward over time; worsening pain or new nerve symptoms needs reassessment.
Can osteoporosis fractures happen without a fall?
Yes. A vertebral compression fracture can occur after bending, coughing, lifting, or twisting if bone density is low enough. A provider may recommend X-ray or MRI when symptoms match a fracture pattern.
Should I exercise after an osteoporosis-related fracture?
Yes, but exercise must match healing stage and fracture location. Early plans often use walking, breathing drills, neutral-spine transfers, hip strengthening, and balance work. Loaded spinal flexion, aggressive twisting, and high-impact activity usually wait until clearance.
What provider should I see for osteoporosis fracture rehab?
A physical therapist can guide gait, balance, strengthening, and safe return to activity. A chiropractor trained in low-force techniques can help with joint mechanics, posture, and movement strategies. Use find a physical therapist near you when mobility, balance, or strength is limited.
- Urgent symptoms need immediate evaluation.
- New pain after a fall deserves screening.
- Known osteoporosis requires modified manual care.
- Fall prevention should start before the next fracture.
What to Do Next
Get evaluated promptly if you have sudden back, hip, wrist, rib, or pelvic pain after a minor fall, twist, cough, or lift. Seek emergency care for inability to walk, severe hip or groin pain, new leg weakness, loss of bladder or bowel control, shortness of breath, chest pain, head injury, or confusion.
Schedule routine conservative care when pain is improving but mobility, posture, balance, or strength remains limited. At the first visit, expect a history of the injury, fracture-risk questions, gait and balance testing, ROM screening, posture assessment, and review of any X-ray, MRI, DEXA, or FRAX information. The provider should ask about prior fractures before using manual techniques.
A safe plan usually starts with protected movement, neutral-spine mechanics, walking tolerance, hip and back extensor strengthening, and fall-prevention drills. Your provider may coordinate with other clinicians if imaging, bone-density testing, or higher-level evaluation is needed.
- Choose PT when walking, transfers, strength, or balance are the main problems.
- Choose low-force chiropractic care when spinal stiffness, posture mechanics, or joint motion need skilled assessment.
- Use both when fracture recovery requires movement retraining plus manual-care modifications.
To start, find a chiropractor near you or explore more health topics on Medximity before your appointment.