The deep neck flexor chin nod exercise is the most direct intervention for retraining the longus colli and longus capitis — the two deep stabilizer muscles most consistently inhibited in people with chronic neck pain, forward head posture, and cervicogenic headaches. Performed correctly, it produces measurable improvements in cervical endurance, pain intensity, and head-on-neck alignment within 4–6 weeks of consistent training.
What Are the Deep Neck Flexors and Why Do They Matter for Neck Pain?
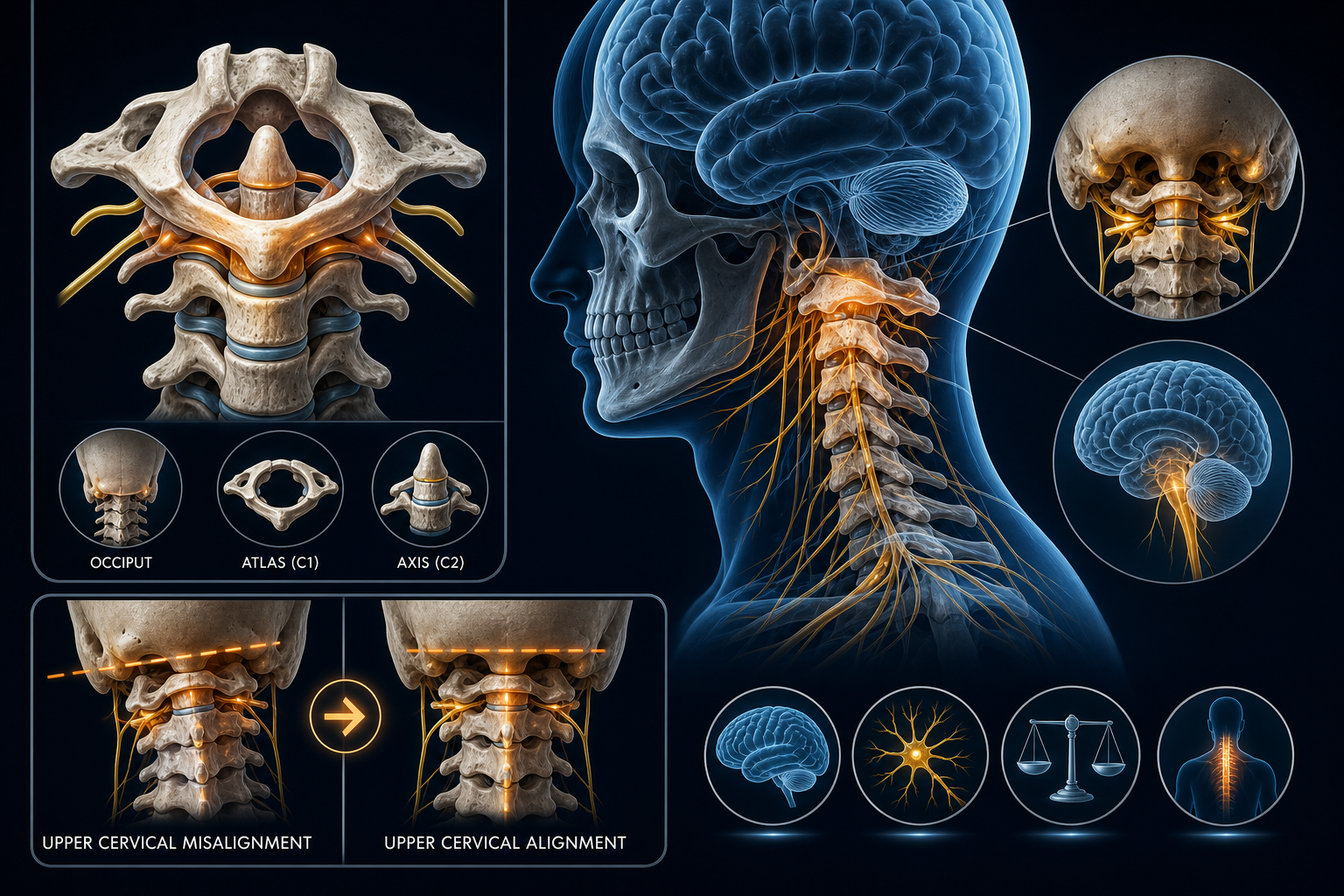
Most neck pain is not a muscle spasm problem — it is a muscle inhibition problem. The longus colli and longus capitis sit directly anterior to the cervical vertebrae (C1–C7) and function as the spine's primary segmental stabilizers. When these muscles are underactive, the sternocleidomastoid and anterior scalenes compensate, creating the compressive, tight-feeling neck pain most people recognize.
Research published in the Journal of Orthopaedic & Sports Physical Therapy found that individuals with chronic neck pain show significantly delayed deep neck flexor activation compared to pain-free controls — meaning the inhibition is neuromotor, not just structural. You cannot stretch your way out of this. You have to retrain the recruitment pattern.
Deep neck flexor weakness is directly linked to:
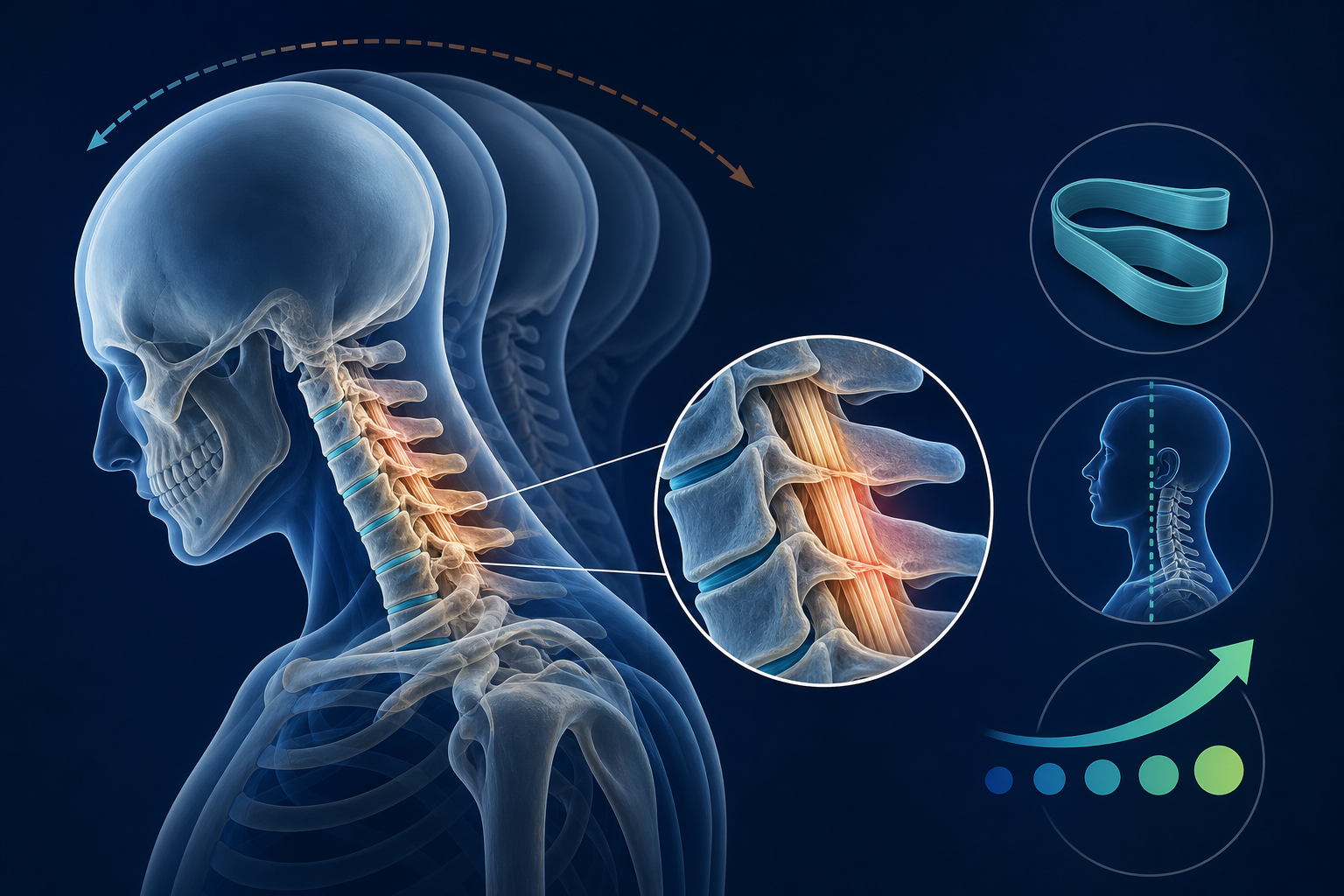
- Forward head posture (every inch of forward translation adds approximately 10 lbs of effective load on the cervical spine)
- Cervicogenic headaches originating from C1–C3 dysfunction
- Whiplash-associated disorder following motor vehicle accidents
- Neck pain from prolonged phone or screen use — the "tech neck" population
Chin Nod vs. Chin Tuck: What Is the Difference?
The difference between a chin nod and a chin tuck is frequently misunderstood, and performing the wrong movement produces the wrong result.
A chin tuck is a gross cervical retraction — you push the entire head backward, compressing the posterior joints and recruiting the superficial flexors. It has a place in rehabilitation but does not specifically target the deep stabilizers.
A chin nod is a subtle craniocervical flexion movement. The head does not translate backward. Instead, the top of the cervical spine (the atlanto-occipital and atlantoaxial joints at C0–C1 and C1–C2) performs a gentle nodding motion — as though you are saying "yes" very slowly and with minimal range. The movement range is approximately 10–12 degrees. That is it.
If your chin travels toward your chest and your whole neck flattens, you are performing a chin tuck. If you feel a subtle, deep contraction at the base of your skull without any surface neck tension, you are performing a chin nod. The distinction determines whether you are training the right muscles.
Who Benefits Most from This Exercise?
Cervicogenic Headache Sufferers
The chin nod exercise directly targets the craniocervical junction — where the rectus capitis posterior minor and the upper fibers of longus capitis attach. For people experiencing cervicogenic headaches originating from upper cervical dysfunction, this exercise combined with chiropractic cervical manipulation typically reduces headache frequency within 3–4 weeks. Studies using the craniocervical flexion test show that people with cervicogenic headaches have significantly lower deep flexor activation pressures than pain-free controls.
Post-MVA and Whiplash Patients
Following a motor vehicle accident, the rapid extension-flexion mechanism of whiplash injury damages the proprioceptive system of the deep cervical extensors and flexors simultaneously. Deep neck flexor retraining is a core component of whiplash-associated disorder (WAD) rehabilitation protocols. It is typically introduced at weeks 2–4 post-injury, once acute inflammation has settled, and progressed over 8–12 weeks alongside manual therapy.
The "Tech Neck" Population
If you experience neck pain when looking down at your phone or working at a screen, your longus colli is likely inhibited by sustained forward head posture. The chin nod is your entry-point exercise — 10 minutes per day produces clinically meaningful results over 6 weeks.
How to Perform the Deep Neck Flexor Chin Nod: Step-by-Step Protocol
Starting Position (Supine)
Begin lying on your back with a thin pillow or folded towel under your head — enough to place your cervical spine in neutral, not flexed. Knees bent, feet flat. Arms resting at your sides.
- Find neutral: Your chin should be neither pointing at the ceiling nor tucked toward your chest. The back of your skull rests evenly on the surface.
- Inhale slowly through your nose, allowing your ribcage to expand.
- On the exhale, begin the nod: Gently draw the top of your head toward the wall behind you by nodding your chin slightly downward. Think "lengthen the back of the neck" rather than "tuck the chin." Movement range is small — 10 to 12 degrees maximum.
- Hold for 10 seconds while breathing normally. You should feel a gentle, deep engagement at the base of the skull. You should NOT feel tension in the front of the throat, the jaw, or the superficial neck muscles.
- Slowly release back to neutral. Do not let the head drop or snap back.
- Rest 5–10 seconds between repetitions.
- Perform 10 repetitions, 2–3 sets, once daily. At week 3, progress to a 10-second hold × 10 reps × 3 sets, twice daily.
Breathing coordination matters. The exhale-to-initiate pattern activates the deep stabilizer co-contraction via diaphragm coupling. Do not hold your breath during the hold phase — that substitutes intra-abdominal pressure for muscular control and defeats the purpose.
Common Errors That Reduce Effectiveness
The most common reason people experience neck strain during this exercise is superficial muscle substitution. The sternocleidomastoid and scalenes are larger and faster to recruit than the longus colli — your nervous system will default to them unless you deliberately prevent it.
- Chin traveling too far toward chest: This converts the chin nod into a chin tuck and brings in the superficial flexors. Keep movement minimal.
- Jaw clenching or tongue pressing hard to palate: Both indicate superficial muscle over-recruitment. Teeth lightly apart, tongue resting.
- Neck veins or throat bulging: You are gripping with the platysma or SCM. Back off and reduce movement range.
- Head lifting off the surface: This adds a gravity-loaded component the deep flexors cannot handle in early-stage rehab. Keep contact with the surface throughout.
- Moving too fast: The deep neck flexors are slow-twitch postural stabilizers. Speed bypasses them. Each nod should take 2–3 seconds of controlled movement.
How to Tell If Your Deep Neck Flexors Are Activating Correctly
Place two fingers lightly on the anterolateral aspect of your neck — alongside the trachea, inferior to the angle of the jaw, over the longus colli region. When the exercise is performed correctly, you should feel a very subtle, deep tension develop without the large superficial muscles hardening under your fingers.
If the SCM (the prominent rope-like muscle running from behind your ear to your collarbone) contracts hard, stop. That is substitution. Reset to a smaller range of motion and try again.
The craniocervical flexion test (CCFT) is the clinical standard for measuring deep neck flexor activation — your physical therapist or chiropractor can perform this with a pressure biofeedback unit to give you an objective baseline and track progress. Most healthy adults activate at 22–24 mmHg above resting baseline; people with chronic neck pain often cannot achieve more than 20 mmHg without substitution.
Progressive Variations to Build Deeper Strength
These deep neck flexor exercises without equipment can be performed at home as you advance through rehabilitation:
Stage Exercise Variation Load Target Timeline 1 — Entry Supine chin nod, 10-sec hold Gravity eliminated Weeks 1–3 2 — Intermediate Seated chin nod against wall Partial gravity Weeks 3–6 3 — Functional Standing chin nod, neutral posture Full gravity Weeks 6–10 4 — Loading Supine chin nod with head lift (2 cm off surface) Gravity-resisted Weeks 8–12 5 — Advanced Standing chin nod with light resistance band External resistance Week 10+Never advance a stage while pain is present or while substitution patterns persist. Premature loading of inhibited muscles increases compressive load on the C4–C5 and C5–C6 disc levels — the most commonly symptomatic in chronic neck pain populations.
How This Exercise Fits Into a Broader Neck Rehabilitation Program
The chin nod in isolation addresses one piece of cervical dysfunction. Research consistently shows that combining deep neck flexor training with manual therapy — cervical mobilization or high-velocity manipulation — produces significantly better outcomes than either approach alone. A typical conservative care protocol for neck strengthening after whiplash injury looks like this:
- Weeks 1–2: Manual therapy (chiropractic or PT) to restore joint mobility at C0–C3; supine chin nod begins at week 2
- Weeks 3–6: Progressive chin nod variations + cervical proprioception training (eye-tracking, balance board)
- Weeks 6–12: Functional loading of deep flexors + cervical extensor strengthening (semispinalis capitis, multifidus)
- Weeks 12+: Return-to-sport or return-to-work activities with maintained home program
This protocol is supported by evidence comparing conservative rehabilitation to surgical outcomes for non-myelopathic cervical dysfunction. For most presentations — including WAD Grade I–II, chronic non-specific neck pain, and cervicogenic headache — deep neck flexor training within a supervised rehabilitation program avoids the need for more invasive care entirely. If you experience headaches alongside neck pain, the connection between the two is worth exploring — the link between headache patterns and spinal dysfunction is well established in the literature. Similarly, tinnitus associated with neck dysfunction is another upper cervical symptom that improves with this type of stabilization work.
What to Do Next
If you have had neck pain for more than 6 weeks, experienced a motor vehicle accident in the last 12 months, or notice headaches accompanying your neck pain, do not rely solely on self-directed exercise. A physical therapist or chiropractor trained in cervical rehabilitation will perform a baseline craniocervical flexion test, identify any contributing joint restrictions, and build a protocol around your specific dysfunction pattern — not a generic one.
Seek care urgently (same day) if you experience:
- Numbness, tingling, or weakness traveling into one or both arms
- Loss of coordination in the hands or changes in gait
- Neck pain following trauma with any neurological symptoms
- Severe headache of sudden onset alongside neck stiffness
These signs indicate possible cervical myelopathy, cord compression, or vascular compromise — conditions requiring immediate medical evaluation, not exercise.
For routine neck pain and postural dysfunction, start the supine chin nod today, and schedule a professional assessment within 1–2 weeks to confirm you are executing correctly and to accelerate your progress.
- Find a physical therapist near you who specializes in cervical rehabilitation
- Find a chiropractor near you for cervical manipulation and deep neck flexor assessment
- Learn more about chiropractic care for neck pain
- Explore more evidence-based health topics on the Medximity blog
Frequently Asked Questions
What are the deep neck flexor muscles responsible for neck pain?
The deep neck flexors are the longus colli and longus capitis, located directly anterior to the cervical vertebrae. They function as segmental stabilizers of the cervical spine. When inhibited — due to injury, poor posture, or disuse — the larger superficial muscles (sternocleidomastoid, scalenes) overwork and generate the compressive pain pattern most people associate with neck pain.
What is the difference between a chin tuck and a chin nod exercise?
A chin tuck is a gross retraction of the entire cervical spine — the head translates backward and the whole neck flattens. A chin nod is a subtle craniocervical flexion at C0–C1 and C1–C2, with approximately 10–12 degrees of movement and no backward head translation. The chin nod specifically targets the deep neck flexors; the chin tuck primarily works superficial cervical muscles.
Is the chin nod exercise safe if I have a herniated disc in my neck?
For most cervical disc herniations (C4–C5, C5–C6, C6–C7) without active myelopathy, the supine chin nod is low-risk because it minimally loads the posterior disc and facet joints. However, you should have a provider confirm your diagnosis and clearance before beginning. If the exercise reproduces arm pain, numbness, or tingling, stop immediately and consult a clinician.
How long until deep neck flexor exercises reduce neck pain?
Most patients performing the chin nod correctly, 2–3 sets daily, report measurable reduction in pain intensity within 3–4 weeks. Postural changes and sustained headache reduction typically emerge at 6–8 weeks. Full cervical stabilizer retraining — to the point where the compensatory superficial muscle overactivity resolves — generally requires 10–12 weeks of progressive training.
Can the chin nod exercise help cervicogenic headaches?
Yes. Cervicogenic headaches are directly driven by upper cervical (C1–C3) joint and muscle dysfunction. The chin nod targets the craniocervical junction and, when combined with manual therapy to the upper cervical joints, reduces both headache frequency and intensity. Clinical trials using the CCFT-guided training protocol report 50–70% reduction in cervicogenic headache days over 8 weeks.
Can I do deep neck flexor exercises at home without equipment?
Yes. All five progressive stages — from the supine chin nod through to the standing variation — require no equipment. A thin pillow or folded towel for the supine position is sufficient. The only exception is the Stage 5 resistance band variation, which requires a light therapy band. Stages 1–4 are fully equipment-free and appropriate for home use.