Cervical Disc Disorder with Myelopathy means a disc problem in your neck is pressing on the spinal cord, not just irritating a nerve or causing local neck stiffness. That distinction matters because spinal cord involvement can affect hand control, walking, balance, reflexes, and coordination, and it deserves prompt evaluation by a qualified provider.
If you are searching for what patients need to know, start here: this condition often develops from disc bulging, disc degeneration, or narrowing around the cervical spine, and the early signs can be subtle. Dropping objects, trouble with buttons, a heavy or unsteady gait, and reduced fine motor control are warning signs worth acting on.
What Is Cervical Disc Disorder with Myelopathy?
What is cervical disc disorder with myelopathy? It is a cervical spine condition where a damaged or degenerative disc contributes to pressure on the spinal cord. The cervical spine includes seven neck vertebrae, labeled C1 through C7, with discs between most levels. When a disc at levels such as C4-C5, C5-C6, or C6-C7 bulges, degenerates, or collapses, the space available for the cord can shrink.
The key structure is the spinal cord itself. A pinched nerve affects one exiting nerve root. Myelopathy affects the cord, which carries signals from the brain to both arms and legs. That is why symptoms can show up below the neck, including hand clumsiness or changes in walking.
Providers also look at nearby anatomy because symptoms rarely come from one structure alone. Common contributors include:
- Intervertebral disc degeneration or bulging
- Arthritic change around the facet joints
- Thickening of supporting ligaments such as the ligamentum flavum
- Narrowing of the central canal around the cord
Research commonly cited in spine care literature shows cervical myelopathy is one of the most frequent causes of spinal cord dysfunction in adults, especially after age 50.
If your symptoms are mainly headaches or upper neck tension, those may overlap with other issues. Medximity has related education on common head pain and migraines, but cervical myelopathy is different because the spinal cord is involved.
How Does Myelopathy Differ From Neck Pain and Radiculopathy?
Cervical myelopathy vs pinched nerve comes down to location. Neck pain is usually local. Radiculopathy involves one nerve root. Myelopathy involves the spinal cord and can affect multiple body regions at once.
Neck pain
Local neck pain often comes from muscles, joints, or discs without major cord compression. The upper trapezius, levator scapulae, and deep cervical extensors commonly become irritated with prolonged desk work, driving, or device use. Pain may stay in the neck and upper shoulder blade region.
Radiculopathy
Radiculopathy usually causes symptoms along one nerve pattern. A C6 nerve root problem may refer symptoms into the thumb side of the forearm. A C7 pattern may affect the middle finger and triceps region. Tingling, burning, or weakness tends to follow a more predictable path.
Myelopathy
Myelopathy is less about one dermatome and more about signal disruption through the cord. You may notice changes in:
- Buttoning a shirt or writing
- Grip release and finger coordination
- Walking speed or balance
- Leg stiffness or a heavy-legged gait
- Reflexes that seem unusually brisk
If you are also dealing with dizziness or balance complaints, compare your symptoms with Medximity’s article on vestibular disorders treatment. Balance loss from the inner ear and balance loss from cervical cord involvement can feel similar at first, but the exam findings differ.
What Are the Common Symptoms and Early Warning Signs?
Early signs of cervical myelopathy often start with function, not pain. Neck pain may be mild or even absent. The more useful question is whether your hands and walking pattern are changing.
Common symptoms include:
- Frequent dropping of keys, cups, or utensils
- Difficulty with zippers, buttons, handwriting, or typing speed
- Numbness or altered sensation in both hands
- Unsteady gait, especially when turning quickly
- Leg stiffness, scuffing the feet, or trouble on stairs
- Neck stiffness with reduced rotation or extension
Neck pain and hand weakness causes vary, but once hand weakness is paired with clumsiness or balance change, providers think beyond simple strain. The cord may not be transmitting signals cleanly through the cervical canal.
Red flags deserve urgent assessment. Seek prompt medical evaluation if you develop:
- Rapidly worsening arm or leg weakness over hours to days
- New trouble walking without support
- Loss of bowel or bladder control
- Major loss of hand function that appears suddenly
- Neck trauma followed by numbness, weakness, or coordination loss
A mild symptom that lasts 6 to 8 weeks is not the same as a symptom that worsens each week. Worsening neurologic function changes the timeline and the urgency.
Some people first notice upper cervical tension or headache patterns. Those can overlap with topics like upper cervical subluxation or upper cervical treatment for balance-related complaints, but hand dexterity and gait change point more strongly toward possible myelopathy.
What Can Cause Cervical Disc Myelopathy?
What causes cervical disc myelopathy? Most cases develop from age-related disc degeneration combined with narrowing around the spinal cord. A disc does not need to rupture dramatically to matter. Gradual loss of disc height can shift loading to the joints and ligaments, slowly reducing canal space.
Common mechanical causes
- Disc bulge or protrusion at C5-C6 or C6-C7
- Disc height loss with segmental instability
- Bone spur formation near the vertebral bodies or facet joints
- Canal narrowing from thickened ligamentum flavum
- Postural loading that keeps the neck in prolonged flexion
Contributing habits and exposures
Daily loading matters. A forward-head posture increases demand on cervical extensors and changes force through the lower cervical segments. Long laptop sessions, phone use with the chin dropped, and driving with the head pushed toward the windshield can all add repetitive strain. These habits do not create every case, but they often worsen symptoms already developing from structural narrowing.
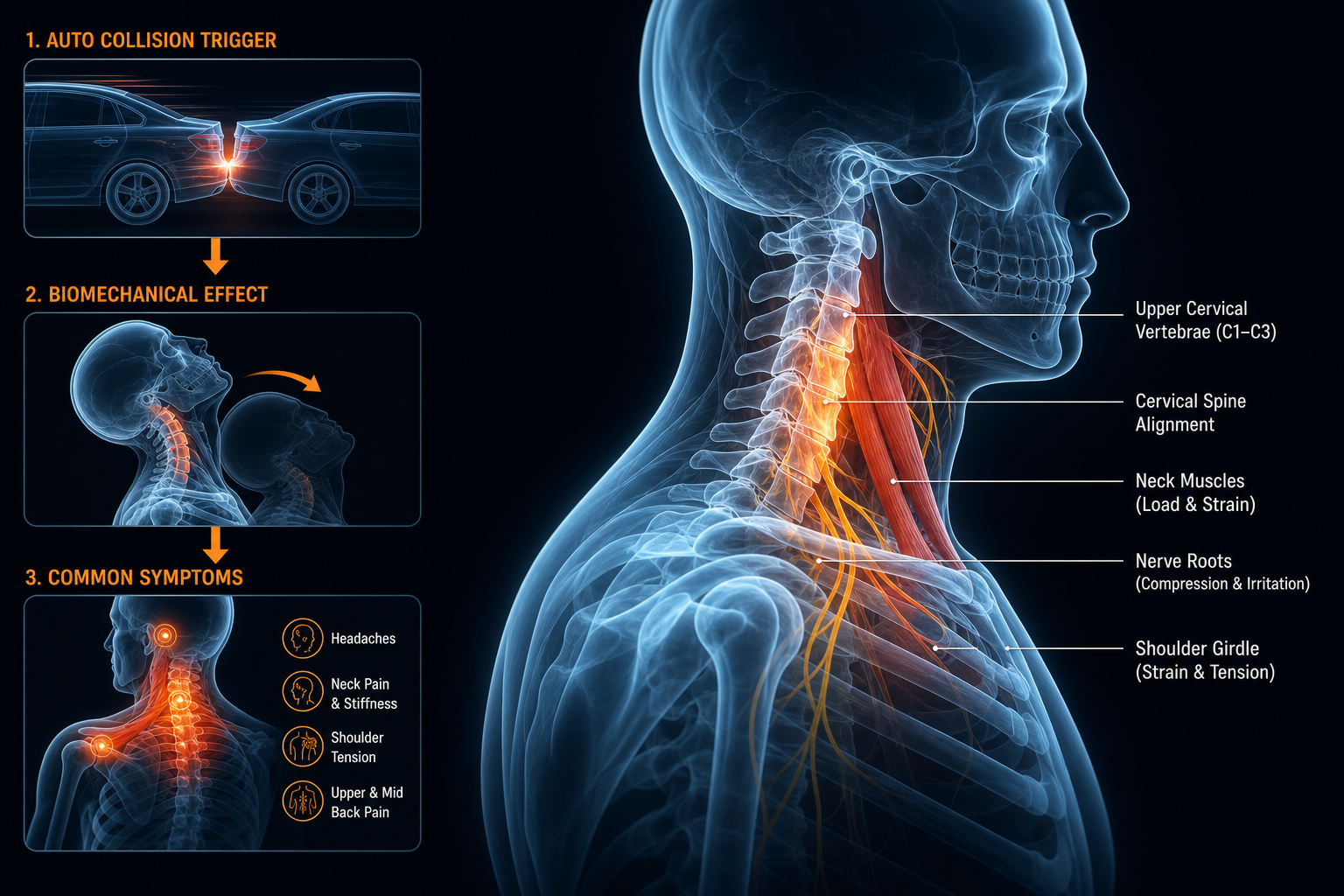
Trauma can also accelerate symptoms. A prior whiplash event, repeated contact stress, or a physically demanding job may uncover a problem that had been silent.
Cause What Happens Common Effect on Function Disc bulge Disc material pushes backward into canal space Neck stiffness, arm symptoms, cord irritation Disc degeneration Loss of hydration and height Segment overload, reduced motion quality Bone spur formation Arthritic overgrowth narrows available space Progressive stiffness and neurologic signs Ligament thickening Support tissues encroach on canal Gait and hand coordination changesHow Do Providers Evaluate This Condition?
How do doctors diagnose cervical myelopathy or determine whether it is likely? They combine your history, a neurological exam, movement testing, and imaging when indicated. No responsible provider should guess based on neck pain alone.
Your first visit usually includes questions about timing and progression. Symptoms present for 2 to 4 weeks after overuse are handled differently than coordination loss that has been slowly worsening for 6 to 12 months.
A provider may assess:
- Cervical ROM including rotation, extension, and flexion
- Grip strength and finger dexterity
- Reflexes in the biceps, brachioradialis, triceps, knees, and ankles
- Single-leg balance, tandem gait, and walking pattern
- Sensation changes in the hands and forearms
- Signs suggesting cord involvement rather than isolated muscle strain
Imaging may be considered if the exam suggests spinal cord compression or if symptoms are progressing. An MRI is often used to look at the disc, the cord, and the amount of space in the canal. X-ray can help show alignment, degenerative change, and disc height loss, though it does not show the cord itself.
A careful exam does two jobs at once: it identifies likely pain generators and it screens for neurologic patterns that should not be managed as routine neck tension.
If your symptoms overlap with dizziness, headaches, or upper neck dysfunction, related Medximity resources on upper cervical chiropractic and quality of life can help you understand adjacent issues, but myelopathy still requires a focused neurological screen.
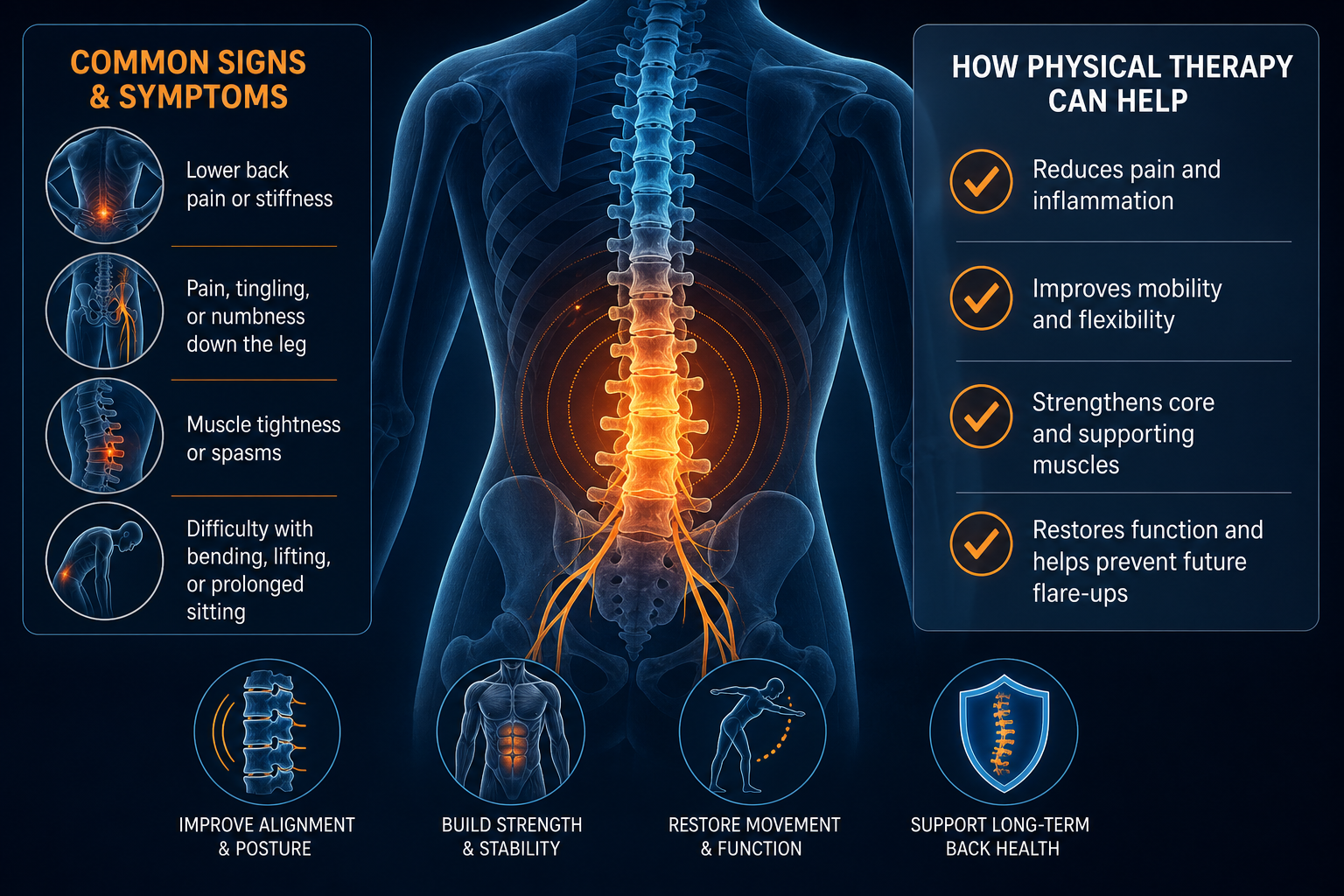
What Conservative Care Options May Help?
Nonsurgical treatment for cervical myelopathy depends on severity, stability, and exam findings. Conservative care is generally considered for mild cases, stable symptoms, or patients being monitored while function remains intact. The goal is not to “push through” cord signs. The goal is to reduce mechanical stress, improve movement quality, and monitor changes closely.
Common conservative options
- Activity modification to reduce repeated neck extension or prolonged flexion
- Physical therapy focused on posture, deep neck flexor control, scapular stability, and gait work
- Chiropractic evaluation to determine what manual care is appropriate and what should be avoided
- Soft-tissue work for overactive muscles such as the upper trapezius, scalenes, and suboccipitals
- Home exercise to restore controlled motion and reduce strain during daily tasks
Cervical myelopathy treatment without surgery must be individualized. In some cases, forceful neck techniques are not appropriate. Providers screen for neurologic progression first. A good plan usually starts with lower-load strategies over 2 to 3 weeks, then rechecks strength, dexterity, and gait before adding more.
Treatment Option Primary Goal Expected Short-Term Outcome Typical Timeline Physical therapy Improve posture, motor control, gait, and endurance Better neck mechanics and daily tolerance Usually 6-8 sessions over 3-4 weeks, then reassess Chiropractic evaluation and selective manual care Identify safe interventions and reduce mechanical irritation Improved mobility in appropriate segments and reduced strain Often 2-4 visits in 2 weeks before formal re-evaluation Posture and ergonomic training Reduce recurring load on cervical discs Less symptom provocation during desk work and driving Daily changes with benefit often noticed within 1-2 weeks Home exercise program Build self-management and movement control Better endurance and less flare with routine tasks Performed 5-7 days per week for at least 4-6 weeksIf lower-body symptoms are also present, compare nerve-related patterns with what can be done for sciatic pain. That article covers a lumbar pattern, but it helps illustrate the difference between local pain and neurologic involvement.
How Can You Reduce Neck Strain Daily?
How to reduce neck strain daily starts with position, duration, and repetition. The cervical spine tolerates movement better than prolonged static postures. Your best strategy is not one perfect posture. It is changing posture before tissues fatigue.
Desk and device setup
- Raise your screen so the top third is near eye level.
- Keep your elbows near 90 degrees and shoulders relaxed.
- Bring the phone to eye level instead of dropping the chin.
- Use a chair that supports the thoracic spine so the head does not drift forward.
Simple home exercise protocol
Use this low-load routine 1 to 2 times per day unless a provider tells you otherwise:
- Sit tall with your ribs stacked over your pelvis.
- Gently draw your chin straight back, creating a “double chin.” Do not tip the head down.
- Hold 3 seconds. Repeat 8 to 10 reps.
- Next, squeeze your shoulder blades down and back without arching the low back. Hold 5 seconds for 8 reps.
- Finish with a doorway pectoral stretch: forearms on the frame, step through slightly, hold 20 seconds, repeat 3 times.
This sequence targets the deep neck flexors, scapular stabilizers, and pectoral tightness that often reinforce forward-head posture. Most people can perform it in under 5 minutes.
Driving matters too. Keep the head against the headrest when possible, bring the seat closer to the wheel, and avoid craning the chin forward. During long drives, stop every 45 to 60 minutes for 2 minutes of walking and posture reset.
When Should You See a Provider Promptly?
When should I see a doctor for myelopathy? See a provider promptly if symptoms suggest cord involvement, especially if they are new, progressive, or affecting hand function and walking. A stiff neck for 3 days after sleeping awkwardly is one category. Progressive clumsiness for 3 months is another.
Schedule a routine but timely evaluation within days if you have:
- Persistent neck pain with numbness in one or both hands lasting more than 1 to 2 weeks
- Fine motor decline such as trouble buttoning clothes or typing accurately
- Balance changes, foot scuffing, or new stair difficulty
- Symptoms that limit work, driving, or exercise despite rest and posture changes
Seek urgent medical care the same day if you have:
- Rapidly worsening weakness in an arm or leg
- Sudden inability to walk normally
- Loss of bowel or bladder control
- Neck injury followed by numbness, weakness, or coordination loss
Neurologic symptoms that are stable for months still deserve evaluation. Neurologic symptoms that worsen over days raise the urgency.
FAQ About Cervical Disc Disorder with Myelopathy
Is it normal to drop things often?
No. Occasional clumsiness happens, but repeated dropping of objects, difficulty releasing your grip, or trouble with buttons and handwriting can be an early sign of cervical myelopathy. If that change lasts more than a few days or is getting worse, schedule an evaluation.
Can cervical myelopathy cause hand weakness without severe neck pain?
Yes. Some patients have mild neck discomfort but noticeable hand weakness, numbness, or loss of dexterity. Because the spinal cord carries signals to the hands and legs, pain intensity does not always match neurologic involvement.
How long does conservative care take?
Timelines vary by severity. A mild, stable case may show better daily tolerance within 2 to 4 weeks of posture correction and guided rehab. Functional retraining often takes 6 to 8 visits over 3 to 4 weeks, followed by reassessment. If symptoms worsen instead of improving, the plan needs review.
Can PT or chiropractic help?
They may help in appropriate cases. PT can improve postural control, scapular stability, gait, and neck mechanics. Chiropractic providers can assess biomechanics and determine whether manual care is appropriate or whether you need a different referral path first. The exam drives the plan.
Does balance trouble always mean an inner-ear problem?
No. Balance trouble can come from the inner ear, the brain, the legs, or the spinal cord. If balance changes occur with hand clumsiness, brisk reflexes, or neck-related neurologic signs, cervical myelopathy should be considered.
What to Do Next
If you suspect Cervical Disc Disorder with Myelopathy: What Patients Need to Know applies to your symptoms, book an evaluation with a provider trained in spine and neurologic assessment. Good starting points include chiropractic, physical therapy, and rehabilitation providers who can screen your neck, reflexes, strength, gait, and coordination, then guide the next step.
At your first visit, expect a history of symptom timing, a movement exam, a neurologic screen, and discussion of whether conservative care is appropriate. Bring a short symptom list with specifics: when symptoms started, whether they are getting worse, what tasks are harder now, and whether walking or hand function has changed.
- For routine evaluation, use Medximity to find a chiropractic near you.
- If you want exercise-based rehab, find a physical therapy near you.
- For broader musculoskeletal support, browse providers or explore more health topics.
If weakness, walking difficulty, or coordination loss is progressing quickly, do not wait for a routine appointment. Seek urgent medical evaluation the same day.