Chiropractor for auto accident treatment usually means early evaluation of the spine, joints, and soft tissues after a crash, then a focused plan to reduce pain, restore ROM, and document injury-related findings. After a rear-end or side-impact collision, the most common problems involve the cervical spine, thoracic spine, lumbar spine, facet joints, surrounding muscles, and supporting ligaments. If you have severe headache, repeated vomiting, loss of consciousness, new weakness, numbness in both arms or legs, chest pain, shortness of breath, or loss of bowel or bladder control, seek emergency care first.
Why see a chiropractor after a car accident?
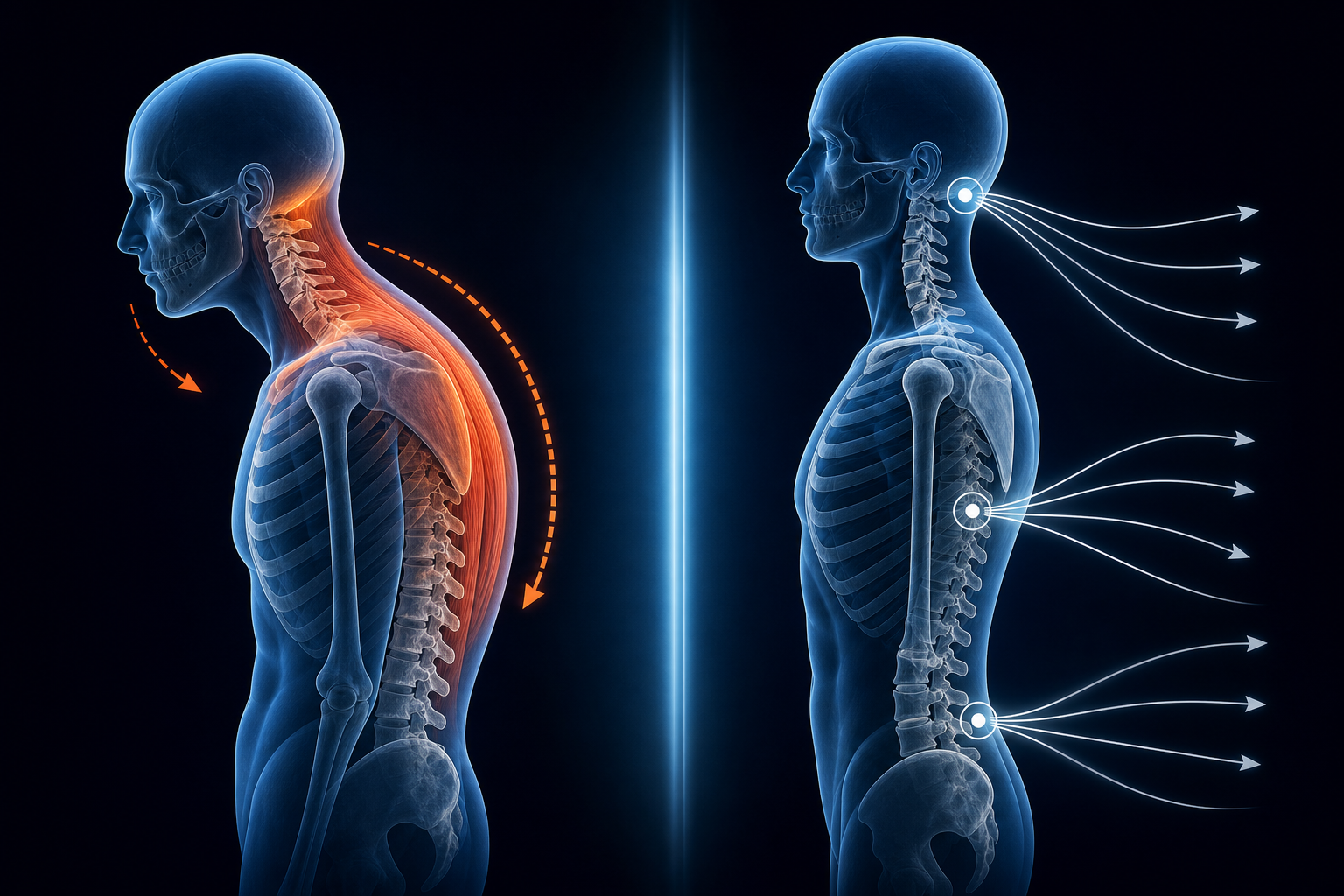
You see a chiropractor after a car accident to identify mechanical injury early, start conservative treatment quickly, and track whether your symptoms are improving or worsening. Low-speed crashes can still overload the sternocleidomastoid, upper trapezius, levator scapulae, scalenes, and the small stabilizers around the neck. Those tissues may tighten within hours, while pain and stiffness often peak at 24 to 72 hours.
Whiplash is not just “neck soreness.” It commonly includes joint irritation, muscle guarding, reduced cervical rotation, headaches from the suboccipital muscles, mid-back pain, rib restriction, and sometimes tingling into the arm if the brachial plexus or cervical nerve roots are irritated.
- Early assessment matters: providers can document ROM loss, muscle spasm, orthopedic test findings, and neurologic changes before patterns become harder to interpret.
- Conservative care fits common crash injuries: spinal manipulation, mobilization, soft-tissue therapy, posture correction, and exercise therapy target the structures most often strained in collisions.
- Function is the goal: treatment should improve turning your head, sitting tolerance, sleep position tolerance, lifting, driving, and work tasks.
- Timelines are predictable: mild strain cases often improve over 2 to 6 weeks, while more involved whiplash patterns may need 6 to 12 weeks of structured care.
Neck pain and low back pain are among the most common complaints after motor vehicle collisions, and delayed onset over the first 1 to 3 days is typical.
If your crash also triggered dizziness, balance problems, or head-pressure symptoms, related post-traumatic patterns may overlap with issues discussed in vestibular disorders treatment and treating post-concussion syndrome by natural means.
What injuries does a chiropractor treat after an auto accident?
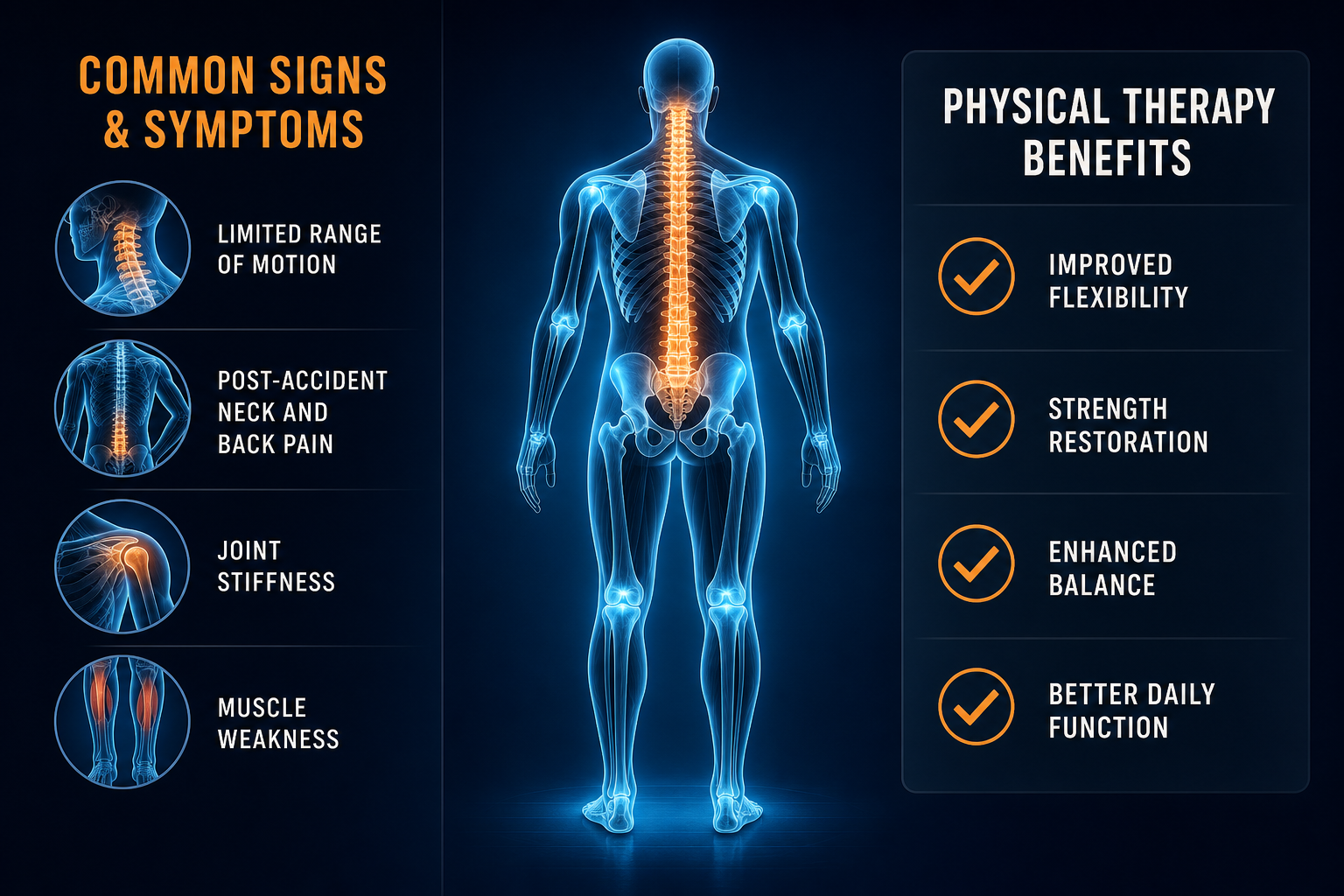
A chiropractor typically treats whiplash-associated disorders, cervical and lumbar sprain/strain, thoracic restriction, rib dysfunction, headache related to neck tension, and nerve irritation that changes strength, sensation, or reflexes. The exact pattern depends on crash direction, seat position, headrest position, and whether your body was rotated at impact.
Common musculoskeletal findings
- Cervical facet irritation: pain with extension and rotation, especially when checking blind spots while driving.
- Lumbar sprain/strain: low back stiffness, pain when rising from a chair, reduced forward bending.
- Thoracic fixation: pain between the shoulder blades, worse with deep breath or prolonged sitting.
- Suboccipital tension headache: pain at the base of the skull that can spread behind the eyes.
- Sacroiliac joint irritation: pain near the belt line, often worse with standing from a seated position.
Symptoms that change the treatment plan
Some symptoms suggest a more complex injury and require co-management or urgent imaging. These include persistent numbness, dropping objects, leg weakness, unsteady gait, visual changes, or severe dizziness with neck movement.
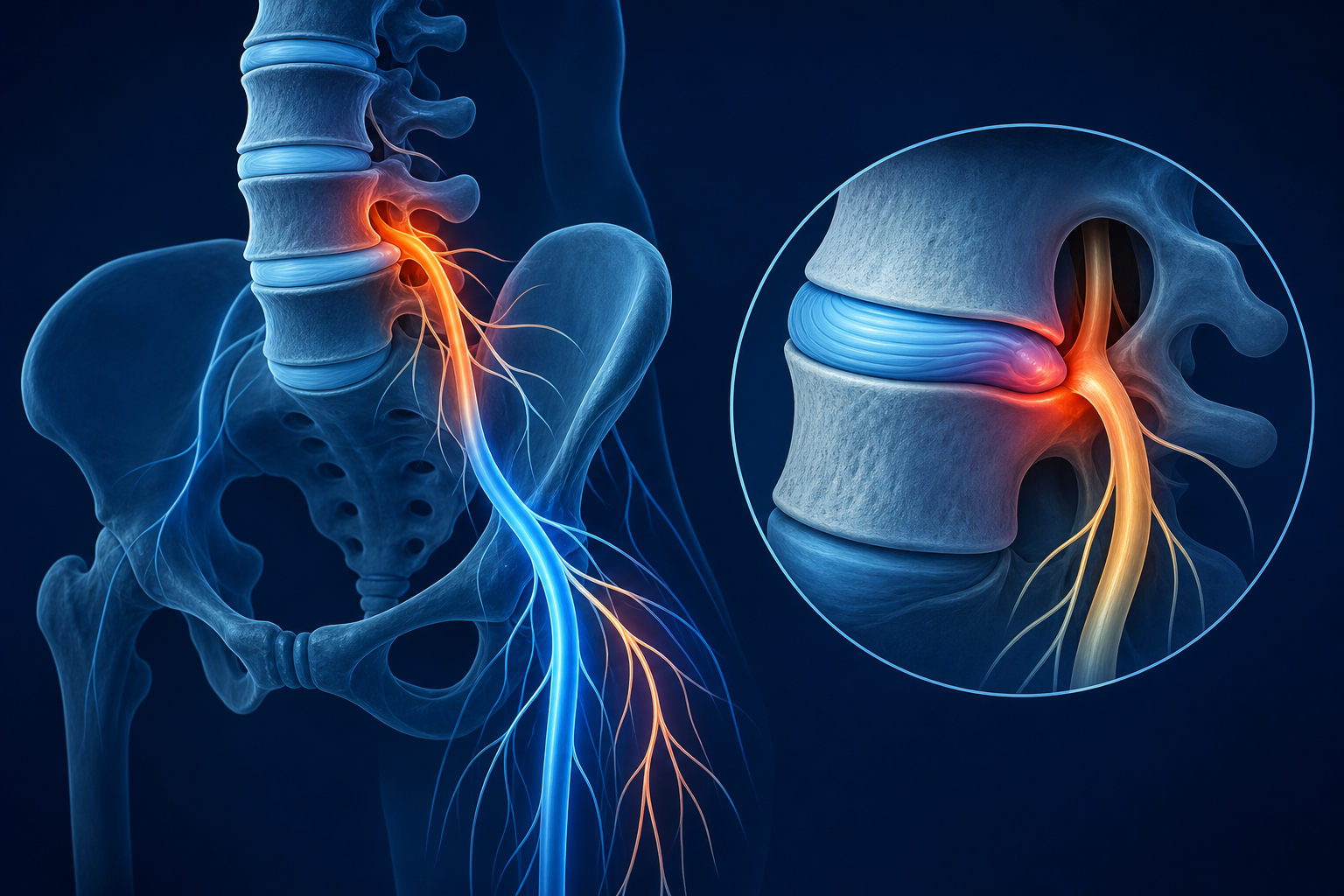
- Radiating arm pain may indicate cervical nerve root irritation.
- Leg pain below the knee may point to lumbar nerve involvement; compare patterns with sciatica treatment and understanding the pain.
- Dizziness or vertigo after impact may reflect cervicogenic dizziness, vestibular dysfunction, or post-concussion changes; see vertigo solution with chiropractic treatment.
Most crash-related cases are treated conservatively first. The key is matching the treatment to the tissue involved instead of using the same visit template for every patient.
What happens at the first chiropractic visit after a crash?
The first visit should establish what was injured, how irritable the tissues are, whether red flags are present, and which movements are safe to begin immediately. Expect a focused history, orthopedic exam, neurologic screen, posture assessment, and ROM measurements of the neck and back.
Exam Component What It Checks Why It Matters After a Crash Active ROM Cervical rotation, flexion, extension, lumbar bending Shows movement loss and pain patterns tied to whiplash or low back strain Neurologic exam Reflexes, sensation, strength Detects nerve irritation or deficits needing urgent follow-up Palpation Muscle spasm, joint restriction, tenderness Identifies involved tissues such as facet joints and paraspinals Orthopedic testing Provocative movement patterns Helps separate disc, joint, muscle, and ligament sources Imaging decision X-ray referral if clinically indicated Rules out fracture or instability when symptoms or mechanism warrant itBring practical details, not a long story.
- Date and type of collision
- Rear-end, front-end, side-impact, or rollover
- Seatbelt use and airbag deployment
- Areas of pain, stiffness, headache, dizziness, tingling, or weakness
- What movements make symptoms worse: rotation, extension, lifting, sitting, coughing
- Any prior neck or back injury
If your headache pattern became frequent after the accident, compare your symptoms with medication free treatment for tension headaches. Crash-related headaches often involve the upper cervical joints and suboccipital muscles rather than a single pain generator.
Can chiropractic care help whiplash and back pain?
Yes, chiropractic care can help whiplash and back pain when treatment is phased correctly: calm the acute irritation first, restore mobility second, then rebuild strength and movement tolerance. Manipulation is one tool, not the whole plan. In the first 1 to 2 weeks, many patients tolerate gentle mobilization, soft-tissue work, supported stretching, and low-load exercises better than high-force techniques.
Early phase: days 1 to 14
- Relative activity modification instead of strict rest
- Gentle cervical and thoracic mobilization
- Soft-tissue treatment for the upper trapezius, levator scapulae, and paraspinals
- Postural correction for sitting, driving, and sleep position
- Light ROM drills several times per day
Recovery phase: weeks 2 to 8
- Progressive spinal manipulation or mobilization as tolerated
- Deep neck flexor retraining
- Scapular stabilization for the rhomboids and lower trapezius
- Lumbar stabilization targeting the multifidus and gluteal muscles
- Work-simulation and lifting mechanics if your job is physical
Typical mild-to-moderate whiplash responds over 6 to 8 visits across 3 to 4 weeks, then tapers if ROM and daily function are improving. More stubborn cases with headache, dizziness, or radiating pain may take 12 to 18 visits over 6 to 10 weeks.
Better outcomes usually come from active care plus manual therapy, not passive treatment alone.
If trauma affected your balance or head position sense, upper cervical findings may overlap with conditions discussed in Meniere’s recovery with upper cervical treatment, though auto-accident evaluation should first rule out post-traumatic causes.
Which treatments work best after a motor vehicle collision?
The best treatment is the one that matches the stage of healing and the structures injured. A patient with acute muscle guarding and limited rotation needs a different plan than a patient 4 weeks out with persistent headaches and weak deep neck flexors.
Treatment Best Use Expected Outcome Typical Timeline Spinal manipulation Joint restriction in cervical, thoracic, or lumbar segments Improved mobility, reduced joint-related pain Often introduced within days to 2 weeks if tolerated Mobilization Acute pain, guarding, low tolerance for force Gentle ROM gains, less pain with turning and sitting First 1 to 14 days Soft-tissue therapy Muscle spasm in trapezius, scalenes, levator, lumbar paraspinals Reduced spasm, better tissue tolerance Useful from first visit through week 6 Exercise therapy Weakness, poor endurance, recurrent pain with activity Longer-lasting stability and function Usually starts in week 1 and progresses for 4 to 8 weeks Posture and ergonomic correction Pain triggered by desk work, driving, sleep position Lower daily aggravation, faster recovery between visits Starts immediatelyPassive care alone rarely solves persistent crash injuries. The best plans usually combine manual treatment with a home program, reassessment every 1 to 2 weeks, and clear functional goals such as:
- Rotate neck 70 to 80 degrees without sharp pain
- Sit 30 to 45 minutes without increased headache
- Drive comfortably for 20 to 30 minutes
- Bend and lift daily objects without lumbar spasm
What can you do at home between visits?
Home care should reduce stiffness without flaring symptoms. The most useful early routine is short, frequent movement instead of long stretching sessions once or twice a day.
Simple 10-minute home protocol
- Chin tuck: Sit tall. Pull your chin straight back without looking down. Hold 3 seconds. Repeat 10 times. This activates the deep neck flexors and reduces forward-head loading.
- Scapular set: Gently pull shoulder blades down and back. Hold 5 seconds. Repeat 10 times. This unloads the upper trapezius and supports the cervical spine.
- Neck rotation AROM: Turn your head right and left only into mild stretch, not pain. Repeat 10 reps each side. Use slow motion.
- Thoracic extension over a rolled towel: Place a towel horizontally under the mid-back while lying on the floor. Support your head with hands. Extend gently 5 to 8 times.
- Pelvic tilt: Lie on your back with knees bent. Flatten the low back into the floor, then relax. Repeat 10 to 15 reps to reduce lumbar guarding.
- Walking: Walk 5 to 10 minutes, 2 to 3 times per day, if symptoms stay stable. Walking improves circulation and decreases stiffness.
Stop the exercise and contact your provider if you get increasing arm numbness, sharp radiating pain, severe dizziness, or headache that escalates rapidly during the drill.
Driving posture matters. Keep the headrest high enough to support the middle of the back of your head, not your neck. Sit close enough to the wheel that your elbows remain slightly bent, and avoid cradling the phone between your ear and shoulder. For athletes returning after a crash, movement retraining principles overlap with sports therapy and whether a chiropractor can improve your game.
When should you worry after an auto accident?
You should worry after an auto accident if symptoms suggest fracture, concussion, progressive neurologic change, or vascular involvement. Most soreness is musculoskeletal. Some findings are not.
- Emergency care now: loss of consciousness, confusion that worsens, repeated vomiting, slurred speech, severe chest pain, shortness of breath, seizure, sudden one-sided weakness, inability to walk, or loss of bowel or bladder control.
- Urgent same-day evaluation: severe headache unlike your usual pattern, constant numbness, dropping objects, marked arm or leg weakness, rapidly worsening neck pain, or severe dizziness after impact.
- Routine but prompt evaluation: stiffness, headaches, back pain, pain with turning, pain between the shoulder blades, sleep-position pain, mild tingling that is not progressing.
Concussion-like symptoms can show up even without direct head strike. If concentration changes, light sensitivity, dizziness, or pressure-type headache developed after the crash, your provider may modify treatment intensity and coordinate further evaluation. Post-traumatic dizziness can mimic inner-ear problems, which is why symptom patterns sometimes overlap with vestibular disorders treatment or upper cervical complaints.
Progressive neurologic symptoms are never a wait-and-see problem.
How long does recovery usually take after chiropractic treatment for a car accident?
Recovery depends on force of impact, prior injury history, tissue irritability, sleep posture, work demands, and whether you start active rehab early. Mild cervical or lumbar strain may settle in 2 to 4 weeks. Classic whiplash with headache and mid-back restriction often takes 6 to 12 weeks. Cases with persistent dizziness, nerve irritation, or delayed treatment can take several months.
Injury Pattern Common Findings Typical Visit Range Usual Recovery Window Mild neck strain Pain, stiffness, mild ROM loss, no neuro deficits 4 to 8 visits 2 to 4 weeks Whiplash with headache Cervical restriction, suboccipital tension, thoracic tightness 8 to 16 visits 4 to 8 weeks Neck and low back injury Reduced bending, sitting intolerance, muscle guarding 10 to 18 visits 6 to 10 weeks Crash-related dizziness or post-concussion features Balance issues, head pressure, motion sensitivity Varies widely 6 weeks to several monthsImprovement should be measurable. Your provider should re-check ROM, pain with specific movements, sitting tolerance, driving tolerance, lifting tolerance, and neurologic findings. If those markers are not changing after 2 to 3 weeks, the plan needs adjustment.
What to Do Next
Schedule an evaluation with a chiropractor experienced in auto accident treatment, whiplash, and active rehab. If your main symptoms are neck pain, back pain, headache, stiffness, or movement loss after a collision, early conservative care is a reasonable first step. Use Medximity to find a chiropractor near you, browse providers, or explore more health topics.
At the first visit, expect:
- A focused history of the crash and symptom onset
- ROM testing of the neck and low back
- Neurologic screening for strength, reflexes, and sensation
- A treatment plan with visit frequency, home exercises, and re-exam timeline
Seek urgent care instead of routine chiropractic care if you have loss of consciousness, worsening confusion, repeated vomiting, major weakness, chest pain, shortness of breath, or loss of bowel or bladder control. For routine musculoskeletal symptoms, get checked within the first few days if possible. Earlier treatment often means fewer compensatory patterns, clearer documentation, and faster return of normal movement.
The goal is not endless visits. The goal is to restore cervical rotation, thoracic mobility, lumbar stability, and daily function with the shortest effective course of care.