Living with a Hip Muscle, Fascia, or Tendon Laceration: A Comprehensive Guide means managing a soft-tissue injury that can change how you walk, sit, climb stairs, sleep, and exercise. A hip muscle, fascia, or tendon laceration involves damage to structures like the gluteus medius, iliotibial band, hip flexor tendons, or deep connective tissue around the pelvis, and conservative rehabilitation often focuses on protecting the tissue, restoring ROM, rebuilding strength, and reducing compensation.
Most mild to moderate soft-tissue hip injuries improve over weeks to months with the right plan. Many patients start with activity modification for 1-2 weeks, then progress through guided mobility and strengthening over 6-12 weeks, depending on depth of injury, tissue involved, and how much limping or weakness is present.
What a Hip Muscle, Fascia, or Tendon Laceration Means
A hip soft tissue injury means some part of the contractile or supportive tissue around the hip has been torn or sharply disrupted. In plain language, a muscle laceration affects the tissue that creates force, a fascia injury affects the connective sheet that helps transmit load and stabilize movement, and a tendon laceration affects the structure that anchors muscle to bone.
If you are asking what is a hip tendon laceration, the simplest answer is this: it is a tear or cut in a tendon near the hip joint, often involving the tendons of the gluteal muscles, hip flexors, adductors, or hamstrings where they attach near the pelvis or upper femur. Tendons tolerate load well, but they heal more slowly than muscle because blood supply is lower.
The hip is not one structure. It is a load-sharing system that includes:
- Gluteus medius and gluteus minimus for pelvic stability when you stand on one leg
- Iliopsoas for hip flexion during walking, stair climbing, and getting into a car
- Adductor longus and related groin muscles for side-to-side control
- Tensor fasciae latae and fascia around the lateral hip for force transfer
- Hamstring origin near the ischial area for bending and pushing off
Clinical rehab often focuses less on the label alone and more on function: Can you bear weight evenly, extend the hip without pain, and control pelvic drop during gait?
That functional view matters because two people with similar imaging findings can move very differently. If you also notice neck tension or balance changes from altered walking mechanics, vertigo solution with chiropractic treatment and other related rehab topics on Medximity can help you understand how body regions influence each other.
How do muscle, fascia, and tendon injuries in the hip differ?
The main difference in a muscle vs tendon injury in hip is where the damage sits and how the tissue behaves under load. Muscle usually hurts with active contraction and stretching. Tendon often hurts when force transfers into bone, especially during repetitive loading. Fascia injuries may create diffuse pulling, stiffness, or a broad band of tenderness rather than one precise point.
Muscle injury
Muscle tissue has better blood flow than tendon, so healing may progress faster. You may feel pain with resisted motion, such as lifting the knee, stepping sideways, or rising from a chair.
- Often sore to stretch and sore to contract
- May bruise or swell earlier after injury
- Typical recovery for a mild strain pattern: 2-6 weeks
Tendon injury
Tendon pain is often more stubborn. You may feel sharp pain at the tendon attachment near the greater trochanter, front of the hip, or groin, especially with stairs, hills, or standing on one leg.
- Less elastic than muscle
- Often aggravated by repeated loading
- Moderate cases commonly need 6-12 weeks of progressive loading
Fascia injury
Fascia spreads force across regions, so symptoms can feel broad and hard to localize. A fascia-related problem may make you feel tight from the lateral hip into the thigh.
Injured Structure Common Location What Aggravates It Typical Early Rehab Focus Muscle Gluteals, adductors, hip flexors Stretching and active contraction Gentle ROM, light isometrics, gait correction Tendon Gluteal insertion, iliopsoas, proximal hamstring Repeated loading, stairs, single-leg stance Load management, progressive strengthening Fascia Lateral hip, pelvic soft tissue planes Twisting, prolonged posture, friction Mobility, soft-tissue work, movement re-patterningWhat causes hip soft tissue injury and what symptoms show up day to day?
The most common causes of hip soft tissue injury are sudden overload, twisting under load, a direct impact, repetitive overuse, or forceful stretching beyond tissue capacity. That can happen during a fall, sports change-of-direction move, lifting with rotation, slipping on stairs, or even aggressive return to exercise after being inactive.
Daily symptoms are usually mechanical. Pain changes with movement, position, and load.
- Hip pain and weakness when walking, especially during push-off or mid-stance
- Limping, short step length, or pelvic drop
- Pain rolling in bed or lying on the involved side
- Sharp pain climbing stairs or stepping into a vehicle
- Difficulty getting socks on because hip flexion or rotation is limited
- Groin pain with pivoting or side-stepping
- Lateral hip pain after standing more than 10-20 minutes
Driving often becomes painful for two reasons: the hip stays flexed too long, and getting in and out combines rotation with weight shift. Getting out of bed can also hurt because you move from trunk rotation into hip loading before the muscles are fully active.
When gait changes, the body often borrows motion from the pelvis and lumbar spine. That is why a hip injury rarely stays “just in the hip.”
If recurrent compensation has started affecting your broader musculoskeletal system, you may also benefit from reading natural fibromyalgia management with chiropractic for a related discussion of persistent movement-related pain patterns.
How does a provider evaluate a hip soft tissue injury?
If you are wondering how do doctors diagnose hip tendon injury, the answer starts with movement testing, not imaging alone. A provider usually identifies the likely structure by asking what motion hurts, where pain is localized, whether you limp, and which tasks fail first: walking, stairs, standing on one leg, bending, or sleeping.
What happens at the first visit
Your evaluation usually includes:
- Observation of walking, sit-to-stand, and single-leg balance
- Palpation of the gluteal tendons, anterior hip, groin, or hamstring origin
- ROM testing for flexion, extension, abduction, and rotation
- Resisted testing of hip flexors, abductors, adductors, and extensors
- Functional screening for pelvic control and lumbar compensation
Why imaging may or may not be needed
Not every hip soft tissue injury needs imaging right away. X-ray helps if bone injury is suspected. MRI may be considered when weakness is marked, the mechanism was severe, bruising is extensive, pain is not improving after several weeks, or a full-thickness tendon injury is suspected.
A skilled PT, chiropractor, or rehabilitation provider can often narrow the problem clinically. Some patients with altered head and neck posture from limping or guarded movement also explore related rehab topics such as Meniere’s recovery with upper cervical treatment or combating cluster headaches with upper cervical care when compensation spreads upward.
What conservative care and rehabilitation options may help?
Physical therapy for hip soft tissue injury usually works best when it progresses in phases. Early care protects the tissue without complete inactivity. Mid-stage care restores ROM and load tolerance. Late-stage care rebuilds strength, balance, and return-to-activity capacity.
Phase 1: Protect and calm the area
- Reduce stride length and avoid painful hills or stairs temporarily
- Use short, frequent walks instead of one long walk
- Avoid aggressive stretching in the first several days if it reproduces sharp pain
- Begin pain-free isometrics such as gentle glute squeeze or standing hip abduction hold
Phase 2: Restore motion and control
- Guided ROM for flexion, extension, and rotation
- Core and pelvic control drills
- Manual therapy or massage therapy for surrounding tone and guarding
- Acupuncture or soft-tissue techniques for pain modulation in some cases
Phase 3: Reload the tissue
- Bridge progressions
- Side-lying or banded hip abduction
- Step-ups with strict pelvic control
- Split-stance loading and gait retraining
For broader rehabilitation topics, you can explore more health topics on Medximity.
How should you walk, sit, sleep, and use stairs with this injury?
How to sleep with hip injury and how to move during the day matter as much as formal rehab. Daily mechanics either calm the tissue down or keep re-irritating it.
Walking should be shorter and smoother, not faster. If you limp after 5 minutes, do 3-4 minute walks more often instead. On stairs, lead with the less painful leg going up and control descent with a handrail until your hip abductors and extensors can accept load normally.
- Sitting: Avoid deep, low seats that keep the hip flexed more than 90 degrees for long periods
- Driving: Slide the seat back enough to reduce hip pinch; pivot your whole body out instead of twisting the leg first
- Sleeping on your side: Place a pillow between the knees and ankles to reduce adduction strain
- Sleeping on your back: Put a small pillow under the knees if front-of-hip tension builds
- Getting out of bed: Roll to your side, drop the legs together, then push up with the arms
Use this simple home protocol once or twice daily if it stays within tolerable pain:
- Lie on your back with knees bent.
- Tighten both glutes for 5 seconds, 8 reps.
- Perform a small bridge, lifting only a few inches, 2 sets of 8.
- Stand and do gentle weight shifts side to side for 60 seconds.
- Finish with 5 slow step-ups on a low step if you can keep the pelvis level.
If symptoms spread into neck tension from altered posture, related resources such as asthma treatment with upper cervical care and three ways to help children suffering with migraines show how regional mechanics can influence whole-body function.
Can a hip injury cause low back pain and problems on the opposite side?
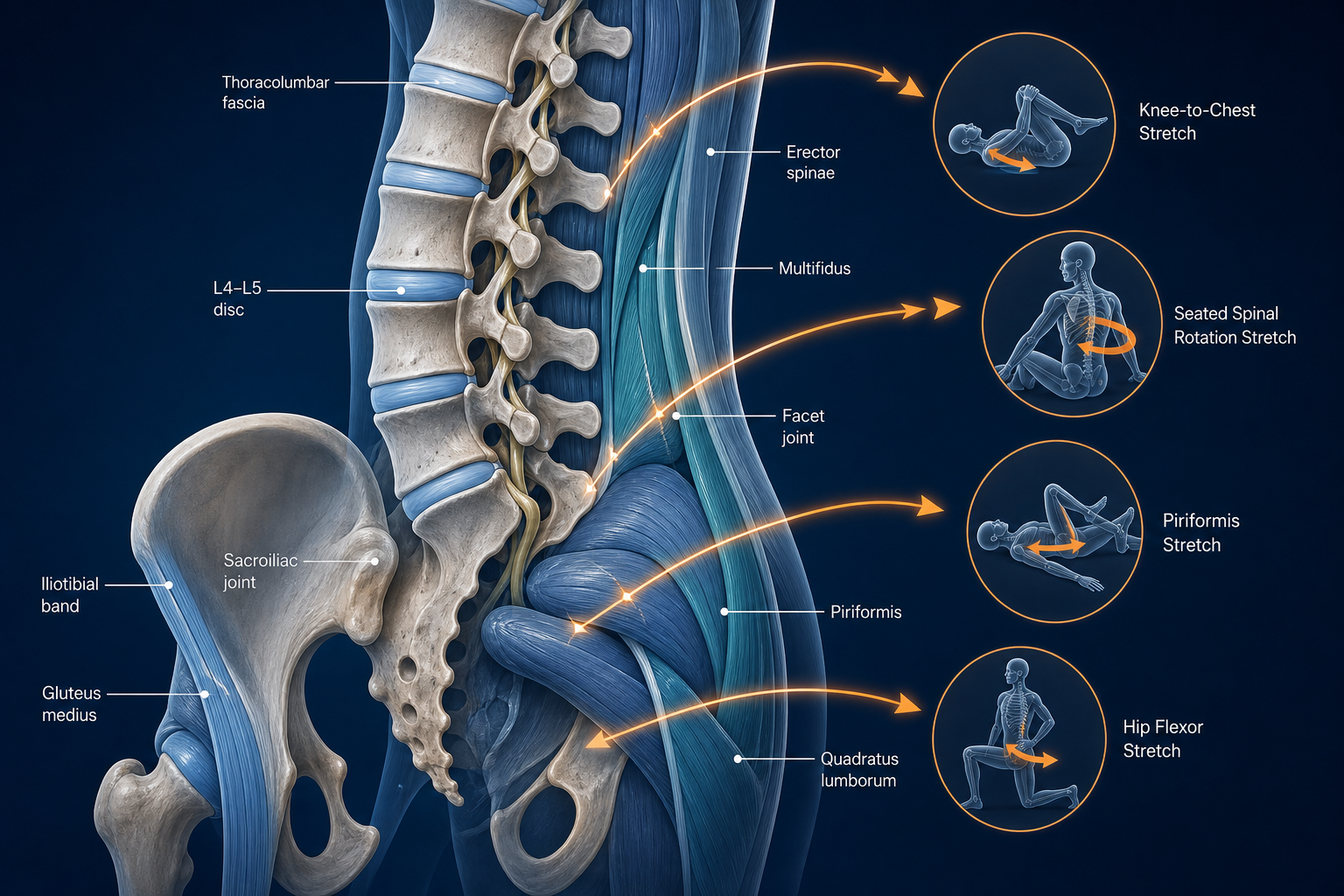
Yes. Can hip injury cause low back pain is a common question because the answer is often yes within days or weeks. When the injured hip stops extending, the lumbar spine extends more. When the gluteus medius cannot stabilize the pelvis, the opposite side works harder during each step. That can produce low back pain, SI region strain, lateral knee overload, or soreness in the “good” hip.
The compensation pattern usually looks like this:
- Shortened stance time on the injured side
- Pelvic drop or trunk lean to avoid loading the gluteals
- Overuse of the quadratus lumborum and lumbar erectors
- Extra demand on the opposite hip abductors and adductors
Left unchecked, compensation can outlast the original tissue injury. That is why rehab should measure function, not just pain. If you can walk with less pain but still drop the pelvis during single-leg stance, the low back and opposite hip may keep absorbing excess force.
One useful checkpoint: you should be able to stand on the involved leg for 10-20 seconds without major trunk lean before returning to more demanding exercise.
When can you return to exercise, and what questions should you ask?
Return to exercise after hip tendon injury should follow function, not impatience. You are usually ready to progress when daily walking is near-normal, stairs are controlled, hip ROM is improving, and basic strengthening no longer causes a next-day flare.
Return-to-exercise progression
- Start with flat walking and controlled bodyweight drills.
- Add bridges, band walks, and low step-ups.
- Progress to split squats, single-leg control work, and longer walks.
- Reintroduce jogging, hills, or lateral movement last.
A practical benchmark is symptom response over 24 hours. Mild muscular soreness is acceptable. Sharp pain, increased limping, or pain that worsens the next morning means the last session exceeded tissue tolerance.
Useful questions to ask about hip injury recovery during evaluation and follow-up visits include:
- Which structure seems most involved: muscle, fascia, or tendon?
- What movements should I limit for the next 1-2 weeks?
- What strength deficit is keeping me from normal walking?
- What home exercises should I do daily, and how many reps?
- What signs show I am ready to return to exercise?
- If progress stalls, what re-evaluation findings would change the plan?
What to Do Next
When to see a doctor for hip injury depends on the pattern. Seek prompt evaluation if you cannot bear weight, heard a pop with immediate weakness, have rapidly increasing swelling, severe bruising, numbness, fever, or pain after a major fall. Seek urgent care sooner if the leg gives out repeatedly or you cannot lift the knee, push off, or stand on the injured side.
Routine but timely care makes sense if you have pain with walking for more than several days, recurring limping, trouble sleeping due to hip position, pain getting in and out of a car, or weakness climbing stairs. Many patients do well starting with a physical therapist, chiropractor, or rehabilitation provider who treats hip and pelvic mechanics. Massage therapy and acupuncture may also be useful adjuncts when guarding and soft-tissue restriction are limiting progress.
- At your first visit, expect a history, movement exam, ROM testing, strength testing, and a plan for home exercise.
- Bring a list of painful tasks: stairs, sitting, driving, sleeping, squatting, and walking distance before limping.
- Track weekly markers: walking time, stair tolerance, side-lying sleep, and single-leg balance.
If you are searching for hip pain physical therapy near me, start here to find a physical therapy near you, find a chiropractic near you, or browse providers. The right conservative plan should explain the injured tissue, reduce overload, restore hip mechanics, and give you a clear week-to-week progression.