How to Get Auto Accident Treatment Covered by UnitedHealthcare / MAHP - MD IPA, Optimum Choice and MLH (formerly MAMSI) usually comes down to three things: which policy is primary, whether your plan requires referrals or prior approval, and whether your provider documents the crash-related diagnosis correctly from the first visit. If you were hurt in a car crash, confirm benefits before care starts when possible, but do not delay urgent evaluation for red flags such as severe headache, weakness, numbness, shortness of breath, or loss of bowel or bladder control.
Will Health Insurance Cover Auto Accident Treatment?
Sometimes yes, but not automatically. If you are asking, will UnitedHealthcare cover car accident treatment, the answer depends on your specific plan, your state rules, whether auto insurance or personal injury protection is primary, and whether the provider is in network.
Coverage for crash-related care often requires coordination of benefits. That means your health plan, auto policy, and sometimes a third-party liability carrier each want to know who should pay first.
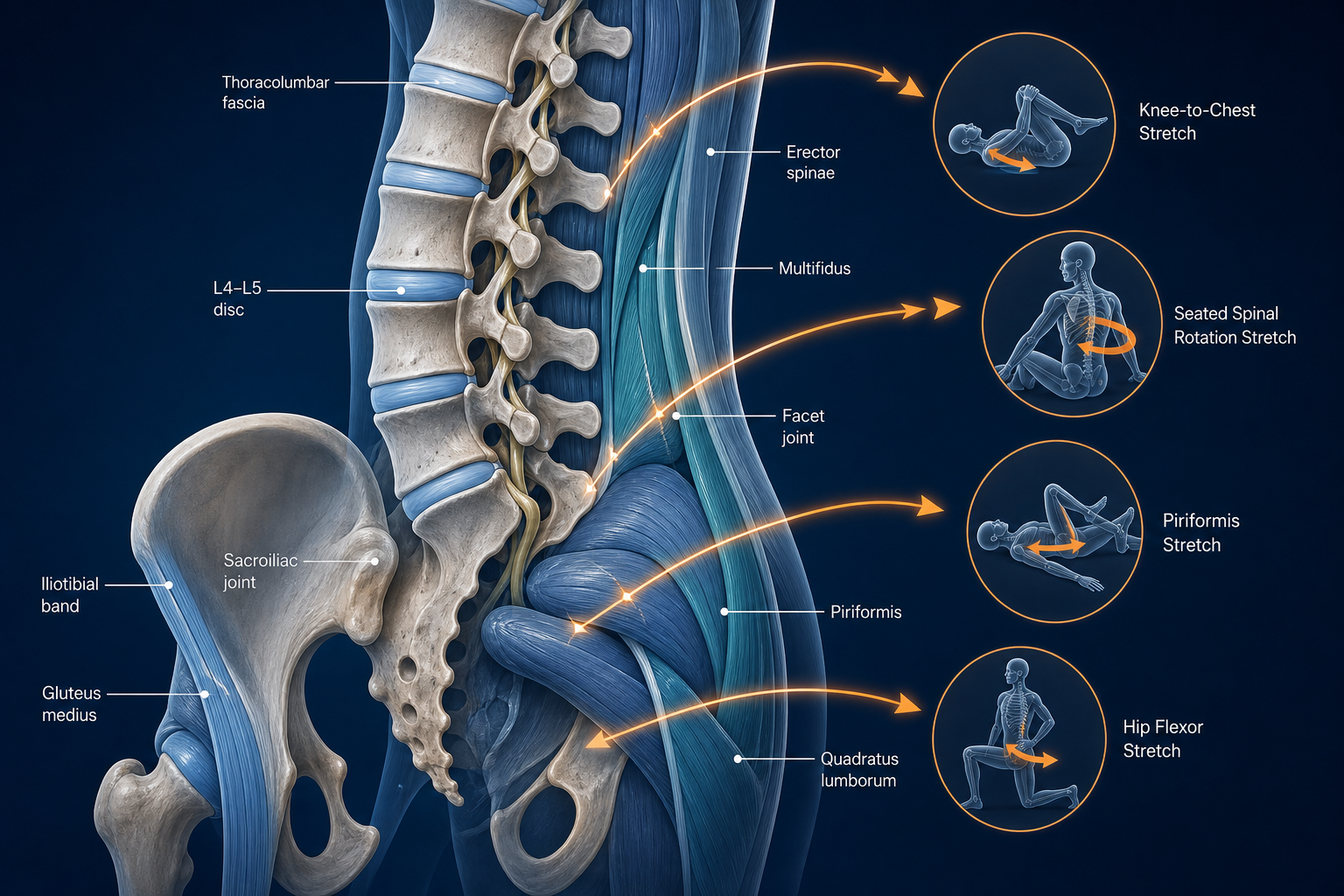
Most crash-related conservative care starts with documented findings involving the cervical spine, lumbar spine, and shoulder girdle. Common diagnoses after a collision include whiplash-associated disorder, neck strain, low back strain, headache, dizziness, radicular pain, and limited ROM. A rear-end crash may irritate the levator scapulae, upper trapezius, and sternocleidomastoid within 24 to 72 hours.
- Health plans may pay after other applicable accident coverage is identified.
- Some managed care plans require a PCP referral before specialty care such as PT or chiropractic.
- Out-of-network benefits may be limited or absent.
- Records must usually connect your symptoms to the date of the crash.
Early conservative care matters. Soft-tissue injuries are often most responsive in the first 2 to 6 weeks, while post-traumatic neck pain and low back pain can linger 8 to 12 weeks or longer if mobility loss is not addressed.
If your crash left you with dizziness, head pressure, or balance issues, related resources like post-concussion syndrome by natural means and vestibular disorders treatment can help you understand what symptoms providers often evaluate after an accident.
How Auto Accident Billing May Work With UnitedHealthcare, MAHP - MD IPA, Optimum Choice, and MLH
Auto accident billing with Optimum Choice plan or other UnitedHealthcare-affiliated products may involve more than one payer. Your provider may ask whether there is MedPay, PIP, bodily injury coverage, or a pending attorney claim before sending the first bill.
What the practice usually checks first
- Date of crash and whether police or incident reports exist.
- Auto insurer name, claim number, and adjuster contact if available.
- Health plan name exactly as printed on your card.
- Whether your plan requires referral, authorization, or in-network use.
- Whether the visit should be billed to health insurance, auto coverage, or placed on hold pending coordination.
Why plan naming matters
Patients often search older plan names. MLH may still be searched under MAMSI. MAHP - MD IPA and Optimum Choice can also involve network and referral rules that differ from broad PPO-style access. The front desk needs the current member ID, group number, and PCP assignment to avoid billing the wrong entity.
Billing Question What It Affects What You Should Ask Typical Delay Risk Is auto coverage primary? Who gets billed first Do you need my claim number before treatment starts? High if missing Do I need a referral? Access to PT, chiropractic, rehab Is PCP approval required for crash-related care? Moderate to high Is the provider in network? Out-of-pocket cost Are these visits covered in network or out of network? Moderate Is authorization required? Visit count and duration How many visits are approved initially? ModerateIf headache patterns began after the crash, some patients also look for options similar to treatment for tension headaches when discussing conservative care with a provider.
How IPA and Managed Care Rules May Affect Your Care
Yes, managed care rules can change where you go and how fast care starts. If you are searching does MD IPA need referral after accident, the practical answer is: often yes for specialty services, but verify with your plan and PCP because rules vary by product and employer group.
An IPA structure usually assigns you to a primary care provider who coordinates specialty access. That affects chiropractic, PT, acupuncture, and rehab more than urgent first evaluation. If you skip the referral step when your plan requires it, the claim may deny even if the treatment itself was reasonable.
- HMO/IPA model: usually tighter network, PCP gatekeeping, referral-sensitive.
- PPO-style model: more direct access, but out-of-network cost may still be high.
- Rehabilitation benefits: may have visit caps, diagnosis rules, or authorization thresholds.
Crash-related musculoskeletal care often targets the facet joints, sacroiliac joints, and supporting muscles such as the multifidus and gluteus medius. A provider may document reduced cervical rotation, lumbar flexion loss, positive orthopedic tests, antalgic gait, or spasm. That level of detail helps establish medical necessity.
Referral problems are one of the most common avoidable billing issues after a crash. One missed PCP authorization can delay several visits.
If leg pain developed after the collision, sciatica treatment and the pain pattern it creates is a useful comparison when you are trying to describe symptoms clearly at intake.
What conservative treatment options are commonly used after a crash?
Car accident treatment without surgery options usually includes chiropractic care, physical therapy, massage therapy, acupuncture, and supervised rehabilitation. These approaches aim to restore ROM, reduce muscle guarding, improve joint mechanics, and rebuild load tolerance.
Common non-invasive options
- Chiropractic care: often used for cervical and thoracic joint restriction, headache, and mid-back or low-back stiffness after whiplash.
- Physical therapy: focuses on ROM, strengthening, posture retraining, and graded return to activity.
- Massage therapy: helps reduce myofascial tone in the upper trapezius, paraspinals, and quadratus lumborum.
- Acupuncture: may be used for pain modulation and muscle tension reduction.
- Rehabilitation exercise: targets deep neck flexors, scapular stabilizers, and core control.
If you are searching chiropractic care after car accident near me or asking whether physical therapy after car accident covered, verify both network status and referral rules before your first full treatment plan is scheduled.
Treatment Best Used For Expected Early Outcome Typical Timeline Chiropractic Neck stiffness, headache, thoracic restriction Improved ROM, less joint-related pain 2-3 visits per week for 2-4 weeks, then reassess Physical Therapy Weakness, guarded movement, return to activity Better movement control and tolerance 6-8 sessions over 3-4 weeks initially Massage Therapy Muscle spasm, trigger points Reduced soft-tissue tension 1-2 sessions weekly for 2-3 weeks Acupuncture Pain modulation, tension patterns Short-term pain reduction in some cases 4-6 visits over 2-3 weeksBalance changes or spinning sensation after impact may overlap with symptoms discussed in vertigo treatment approaches.
How do you verify accident treatment insurance coverage step by step?
If you need to know how to verify accident treatment insurance coverage, use a checklist before or at the first visit. This saves time and reduces denials.
- Call the number on your health plan card and ask whether crash-related care is covered under your specific plan.
- Ask whether auto insurance must be billed first and whether a claim number is required.
- Confirm whether your plan needs a PCP referral for chiropractic, PT, rehab, acupuncture, or massage.
- Ask whether prior authorization is needed after the evaluation or before treatment starts.
- Confirm in-network status for each provider, not just the practice name.
- Ask how many visits are allowed initially and what documentation is needed for more.
- Give your provider the crash date, claim number, adjuster contact, and attorney information if one is involved.
- Request copies of visit summaries and referral approvals.
What to ask the practice directly
- Do you bill auto insurance, health insurance, or both?
- If coverage is delayed, do you offer self-pay or payment arrangements?
- Will you submit records if the insurer asks for medical necessity review?
- Who should I call if a referral is missing?
Keep this process simple: verify the payer, verify the referral, verify the network.
What documentation may help support a claim?
The best documents needed for auto injury insurance claim are the ones created early and kept organized. Insurers look for a clean timeline from crash date to first evaluation to follow-up care.
- Auto claim number and adjuster contact information
- Insurance card images, referral approvals, and authorization numbers
- Initial intake forms stating crash mechanism and symptom onset
- Visit summaries with diagnosis codes and exam findings
- Imaging orders if a provider determines they are needed
- Work status notes or activity restriction notes
- Attendance log showing dates of care
- Receipts for out-of-pocket payments
Detailed exam findings matter. Examples include cervical rotation limited to 45 degrees, lumbar flexion provoking pain into the hamstrings, spasm over the erector spinae, or numbness following a dermatomal pattern. Those findings support why care was necessary and why home exercise alone was not enough at the start.
Simple home protocol to document and follow
- Apply ice wrapped in a towel to the sore area for 10 minutes, up to 3 times daily during the first 48 hours if the area is newly irritated.
- Perform chin tucks: sit tall, draw your head straight back, hold 3 seconds, repeat 10 times.
- Do scapular retraction: squeeze shoulder blades gently together for 5 seconds, 10 reps.
- Walk 5 to 10 minutes twice daily unless your provider restricts activity.
- Write down what movement increases symptoms and what improves them.
That log helps your provider show progress over 1 to 2 weeks and adjust the plan.
Why are claims delayed or denied after accident treatment?
If you are asking why was accident treatment claim denied, the most common reasons are administrative, not clinical. Missing referrals, incomplete accident details, wrong payer order, and weak documentation cause many denials.
How long does accident claim approval take? Straightforward claims may process in a few weeks. Claims involving referral issues, liability review, or missing records can take much longer.
- No referral on file for specialty care
- Provider billed health insurance before required auto coverage information was submitted
- Out-of-network provider used without out-of-network benefits
- Notes do not clearly connect symptoms to the crash
- Gaps in care make medical necessity harder to establish
- Authorization expired before follow-up visits
- Member ID, claim number, or accident date was entered incorrectly
Delays also happen when symptoms suggest a more serious problem. Seek urgent evaluation right away for worsening weakness, foot drop, severe unrelenting headache, repeated vomiting, fainting, chest pain, shortness of breath, or loss of bladder or bowel control. Those are red flags, not routine follow-up issues.
For dizziness or persistent head symptoms after impact, post-concussion care guidance may help you identify what to discuss at re-evaluation.
When should you discuss billing options and legal questions?
Talk with the practice early if coverage is uncertain. A billing conversation on visit one is easier than a surprise balance after six visits.
- Ask whether the practice accepts accident cases under health insurance, auto claim billing, lien-based arrangements where permitted, or self-pay.
- Ask what happens if authorization is delayed after the initial exam.
- Ask whether missed referral rules can be fixed retroactively. Sometimes they cannot.
Speaking with an attorney may make sense when fault is disputed, the auto carrier is unresponsive, wage-loss paperwork is involved, or the amount of care recommended is likely to exceed available accident coverage. That is a legal and financial discussion, not a treatment recommendation.
Your provider’s role is to document exam findings, functional limits, and response to care. The insurer decides benefits. An attorney, if you choose to use one, addresses liability and settlement questions. Keep those roles separate.
What to Do Next
Start with the right provider and the right paperwork. If you have neck pain, back pain, headache, stiffness, or movement loss after a crash, book an evaluation with a chiropractor, physical therapist, or rehabilitation provider who treats collision injuries and understands insurance coordination.
- Use Medximity to find a chiropractor near you.
- Use Medximity to find a physical therapist near you.
- Use Medximity to browse providers or explore more health topics.
At the first visit, expect a history of the crash, ROM testing, orthopedic and neurologic screening, posture and gait assessment, and a discussion of referral or authorization needs. Bring your insurance card, auto claim number, PCP information, and any prior visit paperwork.
Seek routine care promptly if symptoms are mild to moderate and mechanical, such as stiffness, muscle spasm, reduced ROM, or activity-related pain. Seek urgent evaluation now for red-flag symptoms: severe headache, progressive numbness, marked weakness, shortness of breath, chest pain, repeated vomiting, confusion, fainting, or loss of bowel or bladder control.
Benefits vary by policy, network, referral rules, and accident details. Confirm coverage directly with your plan and the treating practice before ongoing care begins whenever possible.
Frequently Asked Questions About Referrals, Out-of-Network Care, Liens, and Coverage Limits
Is it normal to need referral after crash?
Yes. If your plan uses an HMO or IPA structure, a PCP referral for chiropractic, PT, or rehab may be normal even after a car crash. The crash does not automatically remove managed care rules.
Can I see an out of network accident doctor with UnitedHealthcare?
Possibly, but cost depends on your specific plan. If you are searching out of network accident doctor UnitedHealthcare, check whether out-of-network benefits exist and whether the provider will bill your plan directly or require payment at the time of service.
Does coverage include chiropractic and physical therapy after a crash?
Often yes, but only when your policy allows it, the provider is eligible under the plan, and required referrals or authorization are in place. Conservative care is commonly used for whiplash, low back pain, and ROM loss.
How many visits are typically approved at first?
That varies. Some plans approve an evaluation and a short initial block such as 4 to 6 visits, then require progress notes for more. PT plans may start with 6 to 8 visits over several weeks before reassessment.
What if the provider mentions a lien?
A lien is a billing arrangement sometimes used in accident cases when immediate insurance payment is uncertain. Ask the practice to explain it in writing, including your financial responsibility and what happens if the case does not resolve as expected.
What if I still have dizziness, headache, or nerve pain weeks after the crash?
Schedule re-evaluation. Persistent symptoms may require a different rehab plan, further neurologic screening, or a provider with experience in vestibular, post-concussion, or radicular complaints. Medximity also has resources on vestibular disorders and sciatica-type pain patterns that can help you describe symptoms more precisely.