The upper cervical spine is one of the most complex and sensitive regions of the entire musculoskeletal system. Just below the skull, the second and third cervical vertebrae — C2 and C3 — work together to support head movement, protect critical neural pathways, and keep the neck in proper alignment. When those vertebrae shift out of their optimal position, patients may experience a wide range of symptoms that can feel puzzling at first: persistent headaches, a dull ache at the base of the skull, occasional dizziness, or numbness that travels into the shoulders and arms.
If any of those symptoms sound familiar, you are not alone, and the cause may be closer to the top of your spine than you think. This article walks through what C2-C3 neck vertebra misalignment actually is, what may cause it, how it tends to present clinically, and what conservative treatment options — including chiropractic care and physical therapy — may offer.
What Is C2-C3 Neck Vertebra Misalignment?
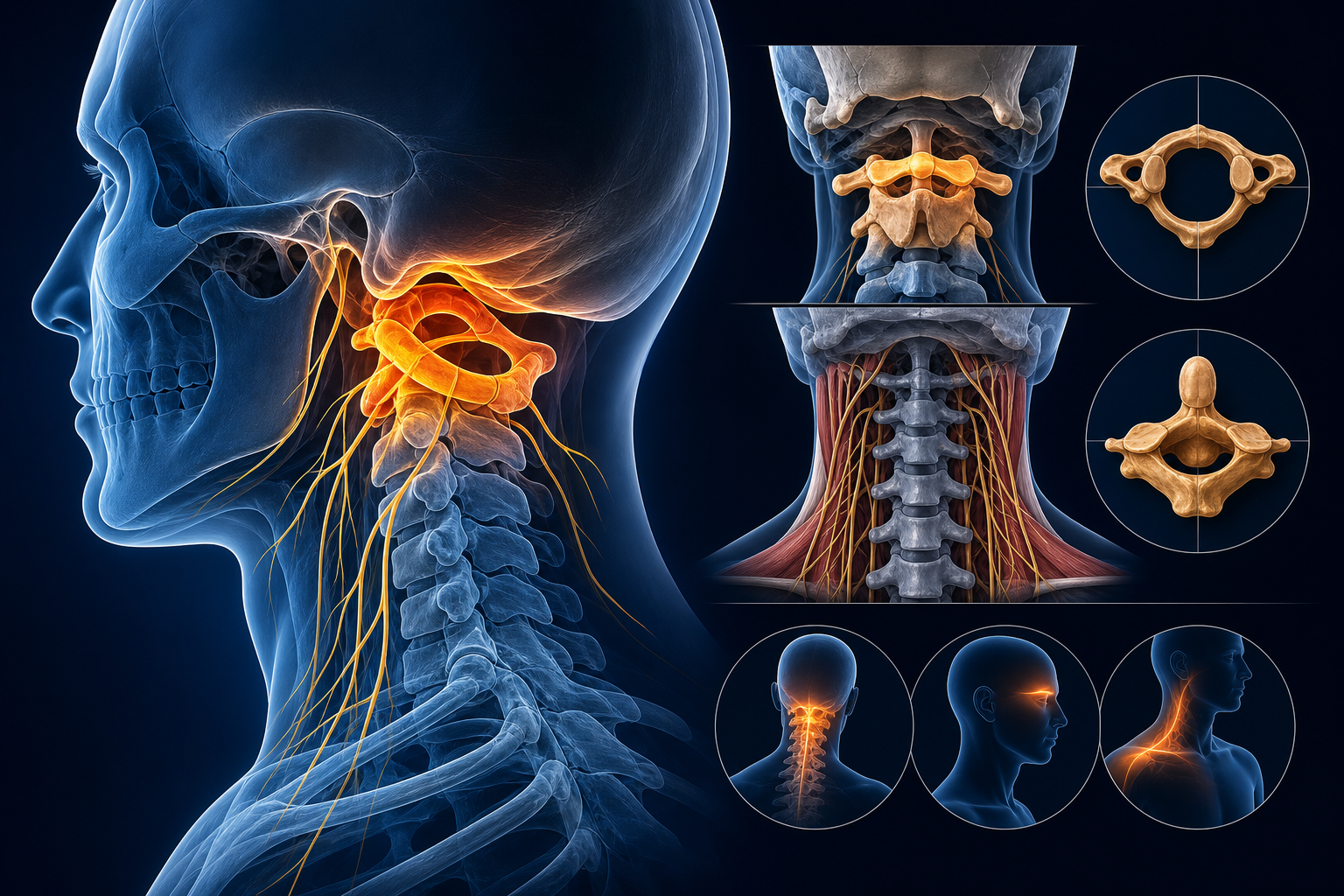
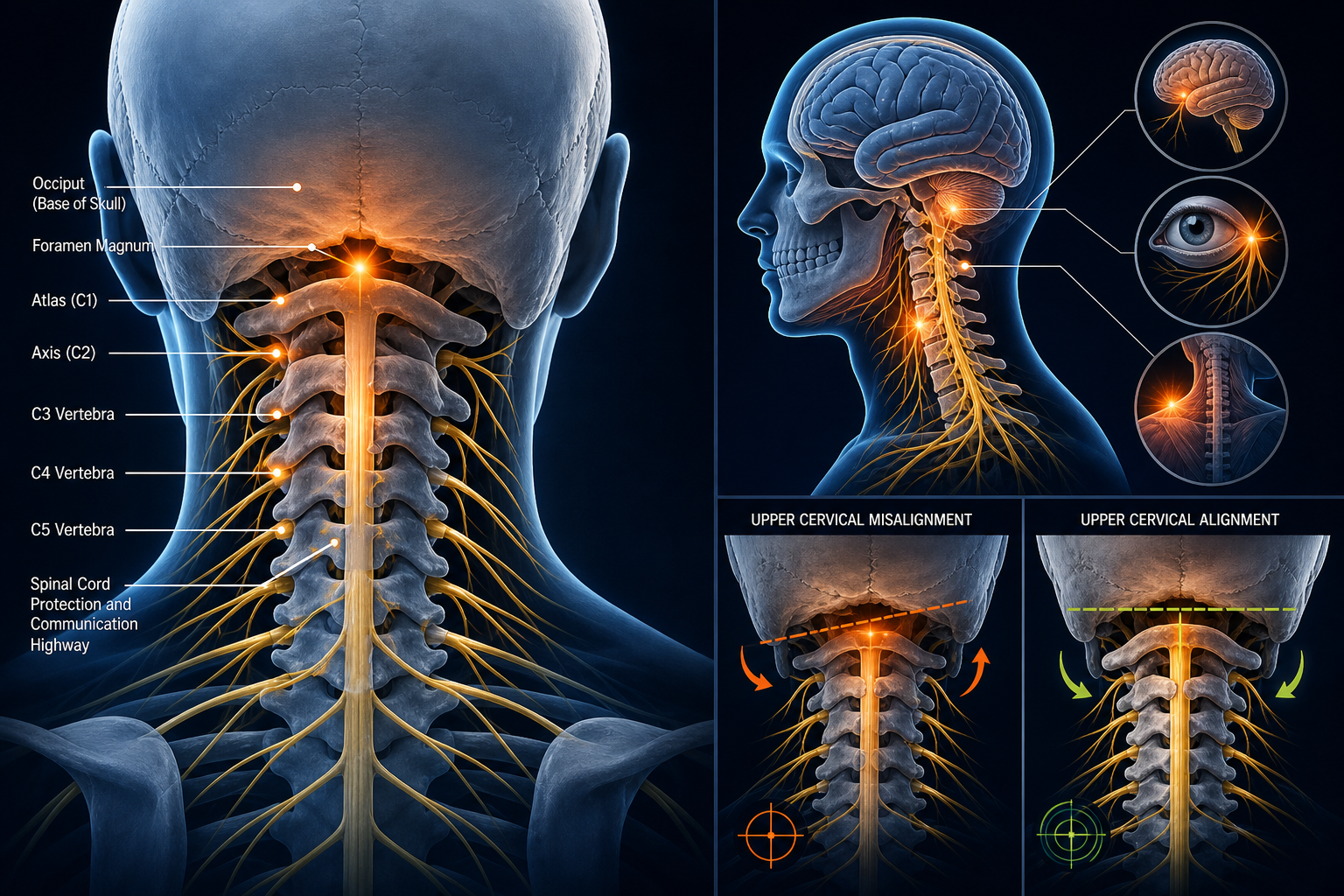
The cervical spine consists of seven vertebrae labeled C1 through C7. The uppermost two, C1 (the atlas) and C2 (the axis), are structurally unique and allow the head to rotate and tilt. C3 sits just below C2 and forms the uppermost segment of what most clinicians consider the mid-cervical region. Together, the C2-C3 segment forms a facet joint — a small, cartilage-lined joint where the bodies of the two vertebrae meet and articulate.
When one or both of these vertebrae shift out of normal alignment — a displacement sometimes called a subluxation or hypomobility — the surrounding structures can be affected. This may include the facet joint itself, the intervertebral disc between C2 and C3, the surrounding muscles and ligaments, and the nerve roots that exit the spinal canal at this level. The C3 nerve root, in particular, is associated with sensation over the back of the head and neck, which helps explain why upper cervical misalignment is so frequently linked to headache patterns.
It is worth noting that the term subluxation carries different meanings depending on the clinical context. In chiropractic practice, it typically describes a vertebral segment that is misaligned or moving abnormally in a way that may affect nerve function. In conventional medicine, the term often implies a more significant partial dislocation. Your provider will clarify what findings mean in your specific case.
Common Symptoms of C2-C3 Misalignment
Because the nerves exiting the cervical spine at the C2-C3 level supply a broad area — from the scalp and base of the skull down through parts of the neck and into the upper shoulders — misalignment at this segment may produce a diverse set of symptoms. Not every patient will experience all of them, and symptoms can vary in intensity and pattern from day to day.
Headaches and Pain at the Base of the Skull
One of the most frequently reported symptoms associated with upper cervical dysfunction is cervicogenic headache — a headache that originates in the neck rather than in the brain or sinuses. This type of headache often begins at the base of the skull and radiates forward, sometimes reaching the temples, forehead, or behind the eyes. Research suggests that irritation of the C2 and C3 nerve roots may contribute to this pattern, though a proper diagnosis is always necessary to rule out other causes.
Neck Stiffness and Reduced Range of Motion
Many patients with C2-C3 involvement notice that turning or tilting the head feels restricted, especially first thing in the morning or after prolonged sitting. Muscle guarding — the body's protective tightening response around an injured or irritated joint — often compounds this stiffness.
Dizziness and Balance Disturbances
The upper cervical spine contains mechanoreceptors — specialized sensory cells that help the brain understand where the head is in space. When normal joint motion is disrupted, some patients report mild dizziness or a sense of being slightly off-balance. This is not the same as the spinning sensation associated with inner-ear conditions like benign paroxysmal positional vertigo (BPPV), but a qualified provider can help distinguish between the two during an evaluation. Learn more about cervicogenic dizziness and how it differs from inner-ear vertigo on Medximity.
Numbness or Tingling in the Arms
A common question patients ask is: can neck vertebra misalignment cause numbness in the arms? The answer depends on the degree of nerve involvement. When a misaligned vertebra or bulging disc places pressure on a nerve root exiting the cervical spine, patients may experience numbness, tingling, or a pins-and-needles sensation that travels down the arm — a pattern called cervical radiculopathy. This symptom warrants prompt professional evaluation, as the degree and location of nerve involvement helps guide the safest and most effective treatment approach.
Upper Back and Shoulder Tension
Chronic tightness between the shoulder blades, or a persistent ache across the top of the shoulders, is frequently tied to upper cervical dysfunction. The muscles that attach in this region often compensate for impaired joint mechanics above, leading to secondary tension that can feel unrelated to the neck at first.
What Causes C2-C3 Subluxation in the Neck?
Misalignment at the C2-C3 level rarely happens from a single dramatic event, though it can. More often, it develops gradually through a combination of physical and lifestyle factors:
- Trauma: Whiplash from a car accident, a sports collision, or a fall can force the upper cervical vertebrae beyond their normal range of motion, sometimes causing misalignment that persists if not addressed.
- Poor posture: Sustained forward-head posture — common with prolonged screen use — places disproportionate mechanical load on the upper cervical spine. For every inch the head shifts forward from neutral, the effective weight the cervical spine must support increases significantly.
- Repetitive strain: Occupational tasks that require the head to be held in a fixed position — looking down at a workbench, turning to monitor equipment, or cradling a phone between the ear and shoulder — can gradually stress the C2-C3 facet joint.
- Sleep position: Sleeping on the stomach with the head rotated to one side for extended periods can stress upper cervical ligaments and joints over time.
- Degenerative changes: As the cervical discs and facet joints age, they may lose height and become less resilient, making the segment more susceptible to dysfunction.
Read more about forward head posture and its effects on the cervical spine on Medximity.
How Is C2-C3 Misalignment Diagnosed?
A thorough clinical evaluation is the starting point. A chiropractor or physical therapist experienced in cervical spine assessment will typically take a detailed history, perform a postural and range-of-motion exam, test neurological function in the arms and hands, and palpate the cervical joints for tenderness or motion abnormalities.
Imaging — most commonly X-rays or, in cases with suspected nerve compression, MRI — may be ordered to visualize vertebral alignment, disc integrity, and any structural changes. However, imaging findings must always be interpreted alongside the patient's clinical picture; many structural changes visible on imaging do not necessarily correspond to a patient's specific symptoms.
Treatment Options for C2-C3 Neck Misalignment Without Surgery
The majority of patients with C2-C3 misalignment are candidates for conservative, non-surgical care. The two most common approaches are chiropractic treatment and physical therapy — and in many cases, a coordinated plan that draws from both disciplines produces the best outcomes.
Chiropractic Treatment for C2-C3 Neck Misalignment
Upper cervical chiropractic care focuses on restoring normal joint motion and alignment to the affected cervical segment. A chiropractor may use a variety of techniques depending on your specific presentation:
- Cervical manipulation (adjustment): A precise, controlled force applied to the C2-C3 segment to restore mobility and reduce joint restriction. Upper cervical techniques tend to use low-force, highly specific adjustments given the sensitivity of this region.
- Instrument-assisted adjusting: Some upper cervical chiropractors use specialized instruments to deliver a gentle, targeted impulse without manual rotation of the neck.
- Soft tissue therapy: Myofascial release, trigger point therapy, or instrument-assisted soft tissue mobilization (IASTM) to address the muscle tension that accompanies joint dysfunction.
- Traction: Cervical traction, applied manually or through a device, may help decompress the joint and reduce nerve irritation in appropriate cases.
Patients often ask: how long does it take to correct neck misalignment? There is no universal answer. Acute cases with no underlying degeneration may respond within a few weeks of care. Chronic or degenerative presentations typically require a longer course of treatment, and the goal in those cases may be functional improvement and symptom management rather than complete correction. Your provider will give you a realistic, individualized estimate after your initial evaluation.
Find a chiropractor near you for upper cervical spine care on Medximity.
Physical Therapy for Cervical Misalignment
Physical therapy approaches cervical dysfunction through movement rehabilitation, neuromuscular re-education, and targeted strengthening. A physical therapist working with a C2-C3 patient may incorporate:
- Cervical joint mobilization: Graded oscillatory movements applied to the cervical joints to restore mobility and reduce pain — different from manipulation but similarly aimed at improving joint function.
- Deep cervical flexor training: Weakness in the small muscles that stabilize the cervical spine from the front is common in patients with chronic neck pain and poor posture. Targeted exercises for these muscles are a cornerstone of physical therapy for cervical conditions.
- Postural correction: Ergonomic assessment, awareness training, and corrective exercises to address the forward-head posture that often perpetuates upper cervical stress.
- Therapeutic exercise: A progressive program to rebuild cervical strength, endurance, and range of motion in a way that supports long-term stability.
Search for a physical therapist who specializes in cervical spine rehabilitation on Medximity.
Physical Therapy vs. Chiropractic for Cervical Misalignment
Both professions have strong evidence supporting their role in cervical spine care, and the choice between them — or the decision to use both — depends on the individual presentation. Chiropractic care tends to focus on restoring joint alignment and mobility through adjustive techniques, while physical therapy emphasizes movement rehabilitation, strength, and functional re-education. Many patients benefit from a collaborative approach, particularly when their condition involves both joint restriction and muscular weakness. Explore a detailed comparison of chiropractic and physical therapy for neck pain on Medximity.
Natural and Supportive Approaches
Alongside professional care, several self-management strategies may support recovery and help prevent recurrence:
- Adjusting workstation ergonomics to keep screens at eye level and reduce forward-head loading
- Using a supportive cervical pillow that maintains neutral neck alignment during sleep
- Gentle range-of-motion exercises as recommended by your provider — not performed without guidance in the acute phase
- Heat or ice applications for temporary symptom relief, as directed by your care team
- Mindful movement practices such as gentle yoga or tai chi, where they have been cleared by your provider
These approaches are supportive, not substitutes for professional evaluation and care. If your symptoms are new, worsening, or accompanied by neurological changes such as arm weakness or coordination problems, seek evaluation promptly.
When to See a Provider
Some neck stiffness and discomfort after a long day at a desk is common. But certain symptom patterns suggest that a professional evaluation should not be delayed:
- Headaches that are new, frequent, or progressively worsening
- Numbness, tingling, or weakness in the arms or hands
- Dizziness or balance problems associated with neck movement
- Neck pain following an accident or fall, even if it initially seems minor
- Pain that has persisted for more than a few weeks without improvement
A chiropractor or physical therapist with experience in upper cervical spine conditions can evaluate your symptoms, identify the contributing factors, and outline a care plan appropriate for your specific situation. Search the Medximity provider directory to find a qualified specialist near you.
Frequently Asked Questions
Is it normal to have headaches from neck misalignment?
Cervicogenic headaches — headaches originating from the neck — are a recognized clinical condition and are commonly associated with upper cervical joint dysfunction, including misalignment at the C2-C3 level. They are not unusual, but they are also not something that should simply be tolerated. A proper evaluation can help determine whether your headaches have a cervical component and whether conservative care may help.
Can neck vertebra misalignment cause numbness in the arms?
Yes, in some cases. When a misaligned vertebra or associated disc places pressure on a cervical nerve root, numbness, tingling, or a pins-and-needles sensation may radiate into the shoulder, arm, or hand — a pattern called cervical radiculopathy. This symptom warrants professional evaluation to assess the degree of nerve involvement and determine the most appropriate treatment approach.
How long does it take to correct neck misalignment?
Recovery time varies widely depending on how long the misalignment has been present, whether there is disc or joint degeneration, and how consistently the patient follows their care plan. Acute cases may show meaningful improvement within a few weeks. Chronic or degenerative cases typically require a longer timeline, and the realistic goal may be functional improvement and sustained symptom relief rather than a complete structural correction. Your provider will give you an individualized prognosis after your evaluation.
What is the difference between chiropractic and physical therapy for C2-C3 misalignment?
Chiropractic care primarily focuses on restoring proper spinal joint alignment and mobility through specific adjustive techniques, including upper cervical adjustments. Physical therapy focuses more on movement rehabilitation, cervical strengthening, postural correction, and functional recovery. Both have evidence supporting their use for neck conditions, and many patients benefit from a coordinated approach that incorporates elements of each. The best fit depends on your specific diagnosis and goals.
Can C2-C3 misalignment be treated without surgery?
In the majority of cases, yes. Chiropractic treatment, physical therapy, soft tissue therapies, and supportive lifestyle modifications are first-line approaches for C2-C3 misalignment and are effective for many patients. Surgical intervention is generally considered only when conservative care has not provided adequate relief and when imaging confirms a structural problem — such as significant nerve compression — that requires it. A qualified provider can help you understand whether conservative care is appropriate for your specific situation.
What causes C2-C3 subluxation in the neck?
Common contributing factors include trauma (such as whiplash from a car accident), prolonged poor posture — especially forward-head posture from screen use — repetitive occupational movements, sleep position habits, and age-related degenerative changes in the disc and facet joints. Often it is a combination of factors rather than a single cause.