A thoracic vertebra dislocation at the T6/T7 level means the sixth and seventh thoracic vertebrae have shifted out of their normal alignment — partially or completely — disrupting the joint surfaces that hold them together. This mid-back injury most commonly results from high-force trauma such as a motor vehicle accident or a significant fall, and it requires prompt evaluation because the spinal cord passes directly through this region.
What Is a Thoracic Vertebra Dislocation?
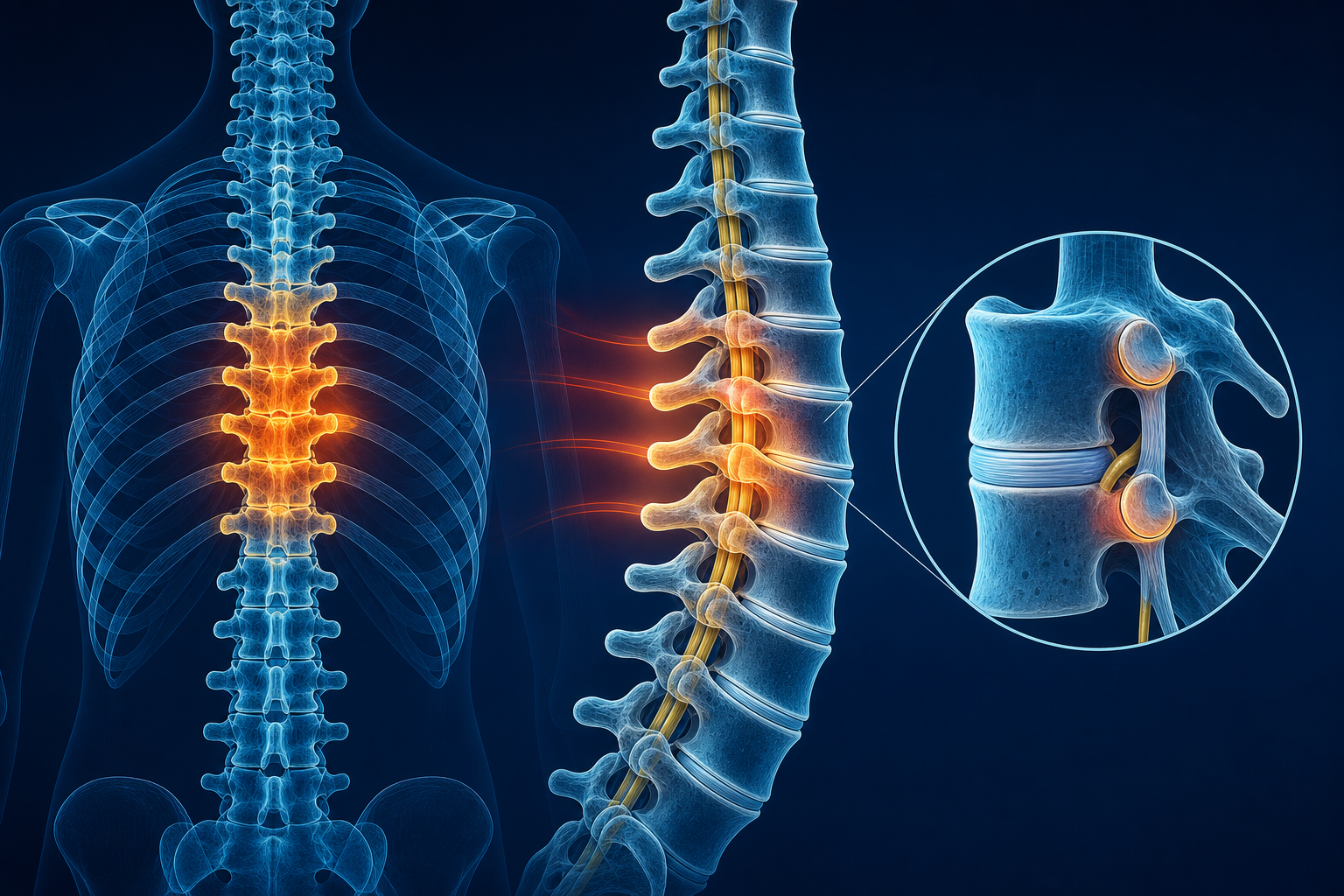
Your thoracic spine is the 12-vertebra segment between your neck and lower back. Each vertebra connects to the one above and below it through paired facet joints and an intervertebral disc. A dislocation occurs when force pushes one vertebra far enough that the facet joint surfaces lose contact with each other. At T6/T7, this means the inferior articular process of T6 displaces relative to the superior articular process of T7.
Unlike a fracture, which breaks bone, a dislocation disrupts the joint relationship itself. In practice, many thoracic dislocations involve both — a fracture-dislocation — but the dislocation component is what threatens spinal cord integrity most directly.
The T6/T7 Region: Why Location Matters
T6 and T7 sit at the midpoint of your thoracic spine, roughly behind the lower border of your shoulder blades. This location has specific clinical significance:
- Rib attachments: T6 and T7 each articulate with their corresponding ribs through costovertebral joints and costotransverse joints. Dislocation at this level often damages these rib connections, which is why rib pain with a back injury at this level is common and expected.
- Spinal cord diameter: The thoracic spinal canal is narrower than the cervical or lumbar canal, leaving less room for the cord. Even a small displacement can compress neural tissue.
- Intercostal nerve roots: The T6 and T7 nerve roots supply sensation to the mid-abdomen and contribute to intercostal muscle function. Injury here can produce a band-like pain or numbness around your trunk at the level of your navel or just above it.
Subluxation vs. True Dislocation: Understanding the Difference
These two terms describe different degrees of the same problem — vertebral misalignment — and knowing the difference between a subluxation and a dislocation of the spine matters for your treatment path.
How They Compare
Feature Subluxation True Dislocation Joint surface contact Partial contact remains Complete loss of contact Ligament damage Stretched or partially torn Typically fully torn Neurological risk Low to moderate Moderate to high Imaging findings Mild offset on X-ray Obvious displacement; MRI shows cord involvement Conservative care role Primary treatment approach Post-stabilization rehabilitationA subluxation is the more common presentation in chiropractic practice — a misalignment that interferes with normal joint mechanics and nerve function but doesn't fully displace the vertebra. A true dislocation involves complete disruption and usually results from significant trauma. If you've been told you have a spinal subluxation, the rehab principles overlap, but the severity and urgency differ substantially.
What Causes a T6/T7 Dislocation?
Mid back pain after a car accident at the T6/T7 level is one of the most common presentations. The thoracic spine is relatively rigid compared to the cervical and lumbar segments, so it typically takes significant force to produce dislocation here.
- Motor vehicle accidents: Rear-end and side-impact collisions generate flexion-rotation forces that concentrate at the thoracolumbar junction and mid-thoracic spine.
- Falls from height: Landing on the back or buttocks transmits axial load upward through the spine.
- Workplace injuries: Crush events, heavy equipment incidents, and falls on construction sites account for a meaningful percentage of thoracic injuries.
- Sports trauma: High-impact sports — football, rugby, equestrian — can generate enough force, particularly with rotational loading.
Research published in the Journal of Orthopaedic Trauma reports that motor vehicle collisions account for approximately 45% of thoracic spine injuries, with falls responsible for another 20-25%.
What Are the Symptoms and Neurological Warning Signs of a T6/T7 Injury?
T6/T7 spinal injury symptoms and treatment decisions depend heavily on whether the spinal cord or nerve roots are involved. Symptoms fall into two categories:
Musculoskeletal Symptoms
- Localized mid-back pain that worsens with movement, coughing, or deep breathing
- Visible or palpable step-off deformity between spinous processes
- Paraspinal muscle spasm along the erector spinae group
- Rib pain radiating along the T6 or T7 intercostal nerve path — wrapping from back to front
- Pain at the costovertebral joints with trunk rotation
Neurological Symptoms to Monitor Closely
Neurological symptoms from a mid-thoracic spine injury demand immediate attention:
- Numbness or tingling in a band-like pattern around your trunk
- Weakness in your legs or difficulty walking
- Changes in bowel or bladder control
- Loss of sensation below the injury level
- Bilateral leg heaviness or coordination problems
Approximately 10-15% of thoracic spine dislocations involve some degree of neurological deficit at initial presentation, according to data from the National Spinal Cord Injury Statistical Center.
Red flag: If you experience sudden leg weakness, loss of bladder or bowel function, or rapidly spreading numbness below your mid-back after trauma, go to the emergency room immediately. These signs suggest spinal cord compression requiring urgent evaluation. Similarly, if you develop new headaches or neck pain alongside mid-back symptoms after a collision, the entire spine needs assessment.
How Is a T6/T7 Dislocation Diagnosed?
Diagnosis relies on a combination of clinical examination and imaging tests. Here is what to expect:
- X-ray: The first-line study. Standing or supine anteroposterior and lateral views can reveal vertebral displacement, loss of normal alignment, and associated rib abnormalities. If dislocation is present, you'll see a clear step-off between T6 and T7 on the lateral view.
- CT scan: Provides detailed bone anatomy and quantifies exactly how much displacement exists. CT also identifies fracture fragments that X-ray might miss.
- MRI: The gold standard for evaluating soft tissue — the spinal cord, intervertebral discs, and posterior ligamentous complex. MRI determines whether the cord is bruised, compressed, or intact, which directly shapes your treatment plan.
Your provider may also perform a focused neurological exam testing sensation in dermatome bands around your trunk, lower extremity strength grading, and deep tendon reflexes at the knee (L3/L4) and ankle (S1) to establish a baseline.
Conservative Care and Rehabilitation Options
Once a provider has confirmed that the dislocation is stable and there is no spinal cord compression requiring emergency intervention, conservative rehabilitation becomes the primary recovery pathway. Chiropractic care for thoracic vertebra injury focuses on restoring proper alignment, joint mobility, and neuromuscular function through a phased approach.
Phase 1: Acute Stabilization (Weeks 1-3)
- Bracing or postural support to limit painful motion
- Gentle soft tissue work to reduce paraspinal spasm
- Ice application: 15 minutes on, 45 minutes off, 3-4 times daily
- Breathing exercises to maintain rib cage mobility without stressing the injury
Phase 2: Guided Mobilization (Weeks 3-8)
- Progressive chiropractic evaluation and gentle spinal mobilization (not high-velocity manipulation in the acute phase)
- Physical therapy focusing on thoracic extension range of motion
- Core stabilization exercises — starting with supine transverse abdominis activation (draw your navel toward your spine, hold 10 seconds, repeat 10 times, 3 sets daily)
- Scapular stabilization work targeting the rhomboids and middle trapezius
Phase 3: Functional Restoration (Weeks 8-16)
- Progressive resistance training for the posterior chain
- Return-to-activity protocols tailored to your work or sport demands
- Ergonomic assessment for workplace setup — particularly if prolonged sitting contributed to or worsens symptoms
If you're also managing radiating nerve pain, the principles used for sciatic-type nerve irritation apply similarly: controlled movement, progressive loading, and nerve glide techniques adapted to the thoracic level.
Recovery: What to Realistically Expect
Thoracic dislocation recovery time without surgery varies based on severity, but here are evidence-based benchmarks:
- Pain reduction: Most patients report 50-60% improvement in resting pain within the first 4-6 weeks with consistent conservative care.
- Functional return: Light daily activities typically resume by week 6-8. Full occupational return for physically demanding jobs averages 12-16 weeks.
- Complete rehabilitation: 4-6 months for most stable dislocations. Some residual stiffness at the T6/T7 segment is common and may persist for up to a year.
- Session frequency: Expect 2-3 visits per week during weeks 1-4, tapering to 1-2 weekly visits through week 12, then biweekly until discharge.
Healing is not linear. You may have setback weeks — this is normal and does not mean your recovery has failed.
Injury Documentation and the Medical-Legal Connection
If your T6/T7 dislocation resulted from an accident — a car crash, workplace incident, or fall on someone else's property — thorough spinal injury documentation for a personal injury claim starts on day one.
- Seek evaluation within 72 hours of the incident. Insurance adjusters scrutinize delays between the accident date and first provider visit.
- Request copies of all imaging — X-ray, CT, and MRI reports with the radiologist's interpretation.
- Attend every scheduled appointment. Gaps in care are used to argue the injury is less severe than claimed.
- Keep a symptom log: Date, pain level (0-10), activities you could not perform, and any neurological symptoms. This contemporaneous record carries weight.
- Ask your provider for narrative reports linking the mechanism of injury (the accident) to the clinical findings. Causation documentation is the backbone of any injury claim.
Providers who regularly work with trauma and accident-related injuries understand the documentation standards that attorneys and insurers require.
What to Do Next
If you have mid-back pain following trauma — especially after a motor vehicle collision, fall, or workplace incident — get evaluated promptly. Specifically:
- Within 24-72 hours of injury: See a chiropractor or rehabilitation specialist for clinical evaluation and imaging referral. Find a chiropractor near you or locate a physical therapist through the Medximity directory.
- At your first visit, expect: A thorough history of the injury mechanism, physical examination including neurological screening, palpation of the T6/T7 segment, and imaging orders if dislocation is suspected.
- Bring to your appointment: Any accident reports, emergency room records, and a written timeline of when your symptoms started and how they've changed.
For ongoing questions about spine conditions, rehabilitation approaches, and provider options, explore more health topics on Medximity.
Frequently Asked Questions
What is a thoracic vertebra dislocation?
A thoracic vertebra dislocation is a displacement of one thoracic vertebra relative to an adjacent vertebra, disrupting the facet joint surfaces that normally hold them in alignment. At T6/T7, this means the sixth thoracic vertebra has shifted out of its normal position relative to the seventh, typically due to high-force trauma.
Is it normal to have rib pain with a mid-back injury?
Yes. Each thoracic vertebra connects to a pair of ribs through costovertebral and costotransverse joints. A dislocation at T6/T7 frequently damages these connections, producing pain that radiates along the rib from your back around to your front, following the intercostal nerve path.
How long does it take to recover from a T6/T7 injury?
With stable dislocations managed conservatively, most patients see significant pain reduction by 4-6 weeks. Functional return to light activities averages 6-8 weeks, and full rehabilitation typically takes 4-6 months. Recovery timelines vary based on severity, age, and consistency with rehabilitation.
How is a spinal dislocation diagnosed with imaging tests?
Diagnosis uses a three-step approach: X-rays to identify alignment changes, CT scans to detail bone anatomy and quantify displacement, and MRI to evaluate the spinal cord, discs, and ligaments. MRI is the most critical study for determining whether neural structures are affected.
Can chiropractic care help after a thoracic vertebra injury?
Chiropractic evaluation is appropriate for stable thoracic injuries. Treatment typically begins with gentle mobilization and soft tissue work during the acute phase, progressing to more active rehabilitation as healing allows. High-velocity adjustments at the dislocation level are generally deferred until adequate healing is confirmed on follow-up imaging.
What neurological symptoms should I watch for after a mid-thoracic injury?
Monitor for numbness or tingling in a band around your trunk, leg weakness, changes in bowel or bladder control, or loss of sensation below the level of injury. Any of these symptoms — especially if they appear suddenly or worsen — require emergency evaluation immediately.