Does Medicare in Georgia cover physical therapy? In many cases, yes. If your physical therapy is ordered and documented as medically necessary, Medicare may help cover outpatient PT in Georgia, but your exact cost, referral requirements, and visit rules depend on whether you have Original Medicare or a Medicare Advantage plan. Before your first visit, confirm that the practice accepts Medicare, ask whether the provider is in network, and verify what you may owe for your evaluation and follow-up visits.
Georgia patients search this question for a simple reason: you want to know whether you can start care for back pain, balance trouble, knee stiffness, shoulder weakness, gait changes, or recovery after an injury without getting surprised by the bill. The federal Medicare rules are the foundation, but the details that affect your real-life access in Atlanta, Augusta, Macon, Savannah, Columbus, or a smaller Georgia community often come down to plan type, provider participation, and documentation.
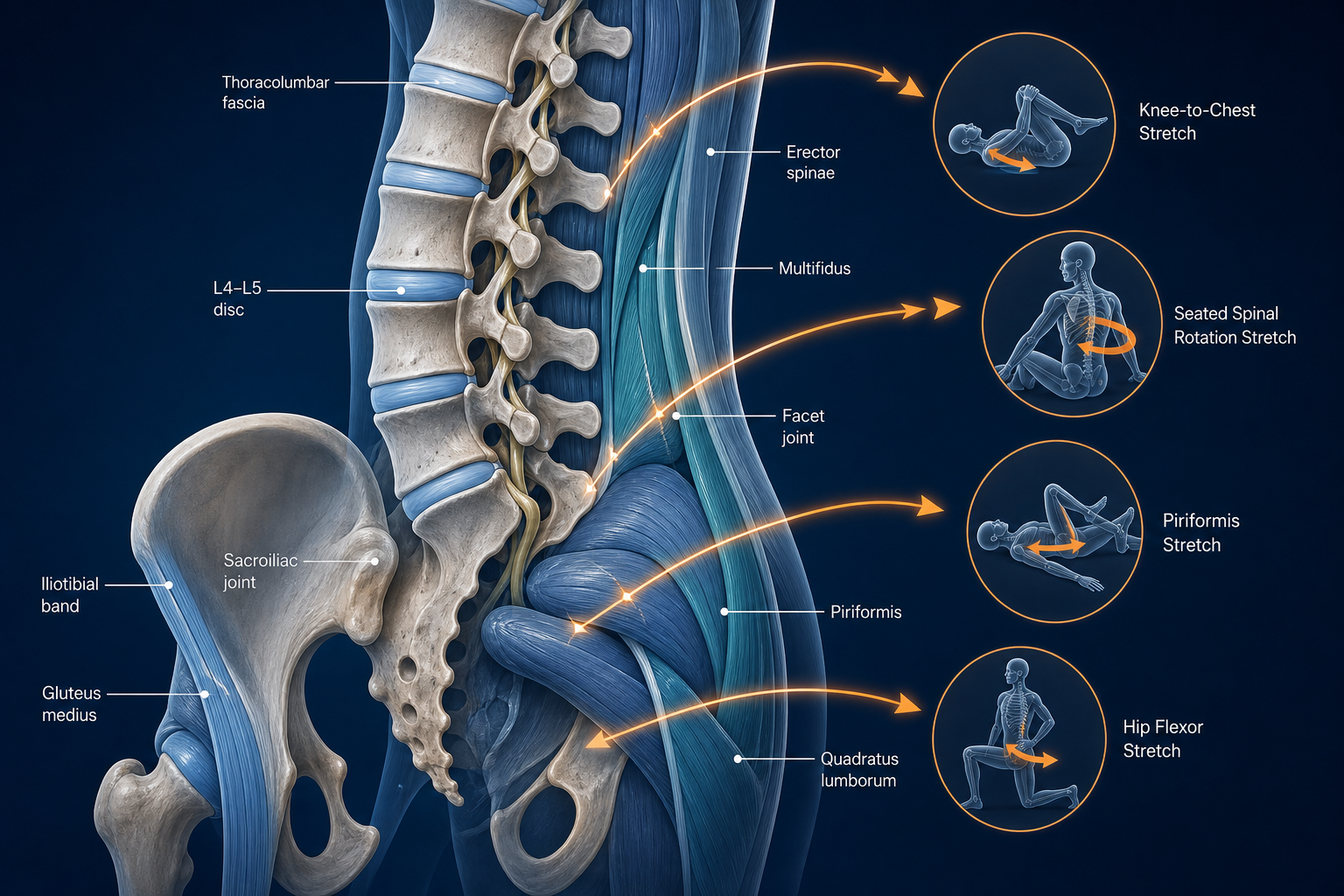
Physical therapy is commonly used to improve ROM, strength, walking tolerance, transfer ability, balance, and functional use of joints such as the shoulder, knee, and hip. It is also used for spine-related problems involving the lumbar discs, sciatic nerve, cervical spine, and surrounding muscles including the gluteus medius, rotator cuff, and quadriceps. Medicare does not pay just because PT sounds helpful. Coverage usually depends on whether your condition creates a measurable functional problem and whether skilled therapy is expected to improve, maintain, or slow decline in a clinically meaningful way.
Does Medicare in Georgia Cover Physical Therapy?
Does Medicare cover physical therapy in Georgia? Usually yes, if the treatment meets Medicare coverage rules and is provided by a qualified practice. The core rules are federal, so Georgia does not create a separate Medicare PT benefit, but your local access still depends on whether the physical therapy practice accepts Medicare assignment, whether your plan uses a network, and whether your care is documented correctly from the start.
For most patients, outpatient PT is the category that matters. That includes care for mobility loss, gait problems, low back pain, neck pain, shoulder dysfunction, knee pain, fall risk, deconditioning, and rehab after an injury. A therapist must evaluate you, identify objective impairments, and create a plan of care tied to function. Medicare generally expects measurable findings such as limited flexion, poor single-leg balance, reduced walking distance, weak hip abduction, painful cervical rotation, or difficulty with stairs, transfers, or daily activity.
Medicare covers outpatient rehabilitation services when they are reasonable and necessary for diagnosis or treatment of an illness or injury and require the skills of a therapist. For patients, that usually means documented functional deficits plus a treatment plan that can be measured over time.
The practical takeaway is simple.
- If you have Original Medicare, outpatient PT is often billed under Part B.
- If you have a Medicare Advantage plan, the plan must cover Medicare-covered services, but it can set different network, authorization, and cost-sharing rules.
- If the practice does not participate with your plan, your cost may be higher or the claim process may change.
- If your records do not show medical necessity, claims may be delayed or denied even if you truly need care.
Patients looking for related rehab guidance often start with the painful area first. If your concern involves leg symptoms or low back pain, see what can be done for sciatic pain and where lower back pain actually comes from. If you are still deciding where to go locally, you can find a physical therapist near you.
What Original Medicare May Cover for Outpatient Physical Therapy
Original Medicare may cover outpatient physical therapy in Georgia when the service is medically necessary, properly documented, and billed by an eligible provider. That usually includes the initial PT evaluation, follow-up treatment visits, periodic progress updates, and in some cases re-evaluation if your condition changes.
What outpatient PT usually includes
Covered outpatient PT may involve hands-on therapy, therapeutic exercise, neuromuscular re-education, balance training, gait training, postural retraining, transfer training, and home exercise instruction. A session may focus on restoring lumbar extension, strengthening the vastus medialis after knee weakness, improving scapular control for shoulder pain, or retraining ankle stability after a fall. Medicare is not paying for general wellness sessions. It is paying for skilled care tied to a clinical problem.
- Initial evaluation with objective measures
- Plan of care with treatment frequency and duration
- Skilled follow-up visits based on functional goals
- Progress reports showing response to treatment
- Discharge planning and a home exercise program
What Original Medicare is looking for in the chart
The chart matters as much as the treatment. The therapist typically needs to show why your condition requires skilled PT rather than unsupervised home exercise alone. That can include documented deficits in gait speed, Timed Up and Go performance, sit-to-stand tolerance, shoulder abduction ROM, trunk endurance, or balance. For example, if you cannot walk more than 200 feet without rest, cannot climb 6 stairs safely, or have cervical ROM too limited for driving checks, those details support coverage more clearly than a vague note that says “pain with movement.”
Service Type What Medicare Usually Looks For Expected Outcome Typical Timeline Initial PT evaluation Diagnosis, function loss, ROM/strength/balance testing, plan of care Determine whether skilled PT is needed First visit Therapeutic exercise Documented weakness, limited ROM, or endurance deficits Improve strength, mobility, daily function Often 4-8 weeks Gait and balance training Fall risk, instability, assistive device need, transfer problems Safer walking and reduced fall risk Often 2-6 weeks Neuromuscular re-education Movement control deficits, poor coordination, postural dysfunction Better movement quality and task performance Often 3-8 weeks Re-evaluation Change in status, lack of expected progress, updated goals Adjust plan of care As clinically neededIf your problem is related to dizziness, head symptoms, or neck mechanics, you may also want to explore migraines and related causes or review common head pain patterns. Those articles can help you describe symptoms more clearly when calling a practice.
What “Medically Necessary” Physical Therapy Usually Means
“Medically necessary” physical therapy usually means you have a specific functional deficit that requires the skills of a physical therapist, and the treatment is expected to produce measurable benefit. Medicare is not asking whether PT might feel useful. It is asking whether skilled therapy is reasonable and necessary for your condition right now.
In practical terms, that often means your therapist can document one or more of the following:
- Limited joint motion, such as shoulder flexion below functional range or reduced knee extension affecting walking
- Strength loss, such as weak gluteus medius causing pelvic drop during gait
- Balance deficit, such as inability to hold tandem stance for a safe duration
- Pain that clearly limits function, such as inability to rise from a chair without using both arms
- Difficulty with tasks like stairs, transfers, dressing, reaching overhead, or community walking
- Need for skilled progression, cueing, manual assessment, or safety monitoring
A common example: lumbar pain with radiating symptoms into the buttock or posterior thigh. If the therapist documents positive neural tension, limited trunk extension, weak hip abductors, reduced walking tolerance, and poor tolerance for bending, PT is easier to justify. If the note only says “back discomfort for a while,” the claim is weaker. That distinction matters for patients asking, “what counts as medically necessary physical therapy?”
Progress also matters. Medicare often expects records to show change over time. That can be less pain during sit-to-stand, increased walking from 5 minutes to 20 minutes, shoulder abduction improving from 80 degrees to 140 degrees, or timed balance improving enough to reduce fall risk. If there is no progress, care may still be covered in some cases when the therapist’s skill is needed to maintain function or slow decline, but the reason must be documented clearly.
For many musculoskeletal conditions, a reasonable starting plan is 6-8 visits over 3-4 weeks, followed by reassessment. More complex balance, gait, or multi-joint cases often run 8-12 weeks with progression based on function.
For spine-related problems, conservative care may include PT, mobility work, and in some cases chiropractic care depending on the diagnosis and plan. If your symptoms are linked to neck alignment questions, see what an upper cervical subluxation is. If pain extends into the face or jaw region, possible causes of face pain may help you recognize patterns worth mentioning during your evaluation.
Do You Need a Referral, Evaluation, or Plan of Care?
You may not always need a referral to be seen by a physical therapist, but Medicare billing often depends on a certified plan of care and documentation that supports skilled treatment. The question “do I need a referral for physical therapy Medicare” has no one-line answer because referral rules, direct access, and plan certification are related but not identical.
What you usually need before treatment starts
The first required step is typically a PT evaluation. During that visit, the therapist measures ROM, strength, balance, gait, pain behavior, joint mobility, and functional limits. The therapist then develops a plan of care that usually includes diagnosis-related goals, visit frequency, expected duration, and the treatment methods to be used. Medicare often requires that this plan be certified by an appropriate provider.
- Call the practice and ask if they accept your specific Medicare plan.
- Ask whether the therapist can evaluate you first or whether they want a referring provider involved before the initial visit.
- Confirm whether the plan of care must be signed before ongoing treatment continues.
- Ask what records to bring: insurance card, identification, imaging report if you have one, and any prior therapy notes.
Why the evaluation matters
The evaluation is where coverage is built. A good PT evaluation documents the body systems involved and the function affected. That might include weakness in the rotator cuff, poor activation of the transverse abdominis, antalgic gait due to reduced knee extension, or impaired vestibular testing if you are dizzy. It also establishes a baseline so later progress can be measured.
Typical first-visit findings that support treatment include:
- Shoulder external rotation weakness affecting lifting
- Cervical rotation limits affecting driving
- Hip abductor weakness causing unstable gait
- Ankle dorsiflexion loss affecting stair descent
- Poor single-leg stance increasing fall risk
If you are recovering from a recent injury, timing matters. For many strains, sprains, and mobility losses, starting PT within 1-2 weeks can help prevent stiffness and compensatory movement. For deconditioning or chronic low back pain, a common care window is 2 visits per week for 4-6 weeks, then taper based on progress. These are examples, not guarantees.
If your symptoms began after a head impact or you have dizziness, headache, vision changes, or concentration changes, review what to do next after a possible concussion. Red flags after head injury should not wait for a routine PT appointment.
How Medicare Advantage Plans Can Work Differently in Georgia
Medicare Advantage physical therapy coverage in Georgia may look different from Original Medicare because private plans can use provider networks, prior authorization, and different cost-sharing rules. The plan must cover Medicare-covered services, but the path to getting PT can be more restrictive or simply more structured.
This is where many patients get tripped up. They hear “Medicare covers PT,” book a visit, and later learn their specific plan requires in-network care or authorization after the evaluation. In Georgia, that can matter even more if you live outside a major metro and your local network is narrow.
Common differences with Medicare Advantage
- Network rules: You may need to use in-network PT practices.
- Authorization: Some plans require approval before a block of visits.
- Visit management: The plan may approve treatment in phases, such as 4 visits first, then review progress.
- Copay structure: You may owe a set copay per visit instead of the standard Part B coinsurance structure.
- Referral expectations: Some plans want a PCP or specialist involved before therapy continues.
A patient in Atlanta with a broad PPO plan may have very different access from a patient in Valdosta or Rome with a tighter HMO network. That is why “medicare advantage physical therapy coverage Georgia” should always be verified with both the plan and the practice.
Coverage Issue Original Medicare Medicare Advantage What You Should Ask Provider choice Often broader if provider accepts Medicare Often network-based Are you in network for my exact plan? Authorization Not usually framed as network authorization May require prior approval or staged approvals Do I need authorization before or after evaluation? Patient cost Part B deductible and coinsurance may apply Often fixed copay or plan-specific cost share What will I owe for eval and follow-ups? Visit management Based on medical necessity and documentation May include visit caps or utilization review patterns How are additional visits approved?If you have balance symptoms, fluctuating dizziness, or neck-related complaints, the provider type may matter as much as the plan. Some patients also compare PT with chiropractic or vestibular-focused care depending on the symptom pattern. For related reading, see Meniere’s recovery with upper cervical treatment and then browse providers by specialty and location.
What Patients May Pay Out of Pocket
How much is physical therapy with Medicare? Your out-of-pocket cost usually depends on your plan type, whether your deductible has been met, your coinsurance or copay, and whether the practice accepts assignment or participates with your Medicare Advantage network.
For patients with Original Medicare, outpatient PT is generally associated with Part B cost-sharing. That often means you may owe the annual deductible first if it has not been met, followed by coinsurance for covered services. If you have secondary coverage, some or all of that patient responsibility may be reduced depending on the policy. For Medicare Advantage, the plan may instead use a fixed per-visit copay, coinsurance percentage, or both.
What changes your cost the most
- Whether your deductible is already met this year
- Whether the PT evaluation and treatment codes are covered as billed
- Whether the provider is in network or participating
- Whether your plan requires authorization for ongoing visits
- Whether you need multiple visits per week for several weeks
A straightforward knee mobility problem after a minor injury may need 4-6 visits over 3 weeks. A balance and gait case with leg weakness and fall risk may need 8-12 visits over 6-8 weeks. The cost to you is not based only on the diagnosis. It is based on plan design and provider status.
Patients often assume the first visit is the only bill that matters. In reality, the bigger financial question is the full episode of care: evaluation plus 4, 8, or 12 visits depending on progress and authorization.
When you call a practice, ask for specifics, not estimates that are too broad to help. Use questions like these:
- Do you accept assignment for Original Medicare or are you in network with my Medicare Advantage plan?
- What is my expected responsibility for the initial evaluation?
- What is my expected responsibility per follow-up visit?
- Will you verify benefits before my first appointment?
- Will I be told if authorization is still pending?
If your symptoms involve chronic widespread pain and you are comparing PT with other non-pharmaceutical options, this guide for fibromyalgia patients seeking natural treatment may help you ask sharper questions about function-based care.
Why Claims May Be Delayed or Denied
Why did Medicare deny physical therapy? The most common reasons are missing documentation, lack of medical necessity in the record, network or authorization problems with Medicare Advantage, or a mismatch between the diagnosis, treatment, and documented functional goals.
Most denials are administrative or documentation-related, not proof that PT was the wrong choice. The claim may be held because the plan of care was not certified, progress notes were incomplete, authorization was missing, or the practice billed under the wrong participation status. Patients often do not hear any of this during scheduling, so it helps to ask early.
Common denial triggers
- No clear functional deficit documented
- Plan of care missing required certification
- Visits continue without progress reports
- Treatment looks like general fitness rather than skilled therapy
- Medicare Advantage authorization not approved in time
- Provider is out of network for the plan
- Patient information or insurance data entered incorrectly
Example: if your chart says “back pain, exercises performed” for six visits, coverage is weak. If the chart says “lumbar flexion limited, positive neural tension, hip abduction 3+/5, walking tolerance 7 minutes, goal to reach 20 minutes for community mobility,” the service is easier to defend. Medicare wants measurable function.
You should also know when a PT issue is not routine. Seek urgent medical evaluation rather than routine rehab scheduling if you have any of these red flags:
- New loss of bowel or bladder control
- Rapidly worsening leg weakness or foot drop
- Sudden facial droop, arm weakness, or speech changes
- Severe headache after head injury with vomiting or confusion
- New seizure activity
Those symptoms need immediate evaluation. If seizures are part of the picture, review possible seizure causes to understand why routine PT scheduling is not the first step.
If your claim is delayed or denied, do this in order:
- Ask the practice what specific reason code or documentation issue was flagged.
- Ask whether the denial was due to authorization, provider network status, or chart documentation.
- Confirm that your insurance ID, plan name, and effective dates were entered correctly.
- Ask whether a corrected claim, plan of care certification, or additional records are being submitted.
- Request a written estimate for any balance you may owe while the issue is under review.
Questions to Ask a Physical Therapy Practice Before Your First Visit
The best way to avoid coverage confusion is to ask the right questions before your first appointment. Patients searching “questions to ask physical therapist before first visit” usually need both insurance questions and clinical questions. Ask both.
Insurance and billing questions
- Do you accept Original Medicare, and do you accept assignment?
- Are you in network with my exact Medicare Advantage plan?
- Do I need a referral, authorization, or signed plan of care before treatment continues?
- Will you verify my benefits before the evaluation?
- What is my expected cost for the evaluation and each follow-up visit?
Clinical questions that matter
The practice should be able to explain how they evaluate your specific problem. That is a good sign that the care will be targeted and well documented.
- Will my first visit include ROM, strength, gait, and balance testing?
- How will you measure progress?
- What home exercises will I start with?
- How many visits do patients with this problem typically need?
- What would make you refer me back for a different evaluation?
Ask for a practical timeline. For example, mild shoulder impingement with limited overhead reach often responds over 4-6 weeks. A balance program for recurrent falls may take 6-10 weeks. Low back pain with deconditioning often starts with 2 visits per week for 3-4 weeks, then reassessment. Those are common patterns, not promises.
Also ask what you should wear and bring. Bring your insurance card, photo ID, prior imaging reports if available, a written list of your main functional problems, and any assistive device you use for walking. Wear clothing that lets the therapist examine the joint involved. If your issue is knee pain, tight jeans slow the exam. If your issue is shoulder ROM, a loose shirt helps.
A strong first visit should answer three questions: what structure is impaired, what function is limited, and what measurable change the therapist expects in the next 2-4 weeks.
What to Do Next
If you think you need physical therapy in Georgia, contact a Medicare-participating PT practice now and verify your benefits before the first visit. Do not wait until after the evaluation to ask about network status, authorization, or expected cost.
Start with the right provider type. For walking difficulty, balance problems, post-injury stiffness, shoulder weakness, knee pain, or low back pain limiting daily activity, a physical therapist is usually the right first call. If your symptoms center on spinal mechanics, posture, or non-invasive care for back or neck pain, you may also compare options and find a chiropractor near you. If you are still sorting out the symptom pattern, you can explore more health topics before scheduling.
Here is a simple step-by-step checklist for Georgia patients looking for physical therapy that accepts Medicare near them:
- Find a local PT practice and confirm it accepts your exact Medicare coverage.
- Ask whether you have Original Medicare or a Medicare Advantage network requirement.
- Ask if you need referral input, authorization, or plan-of-care certification.
- Request your estimated evaluation and follow-up visit cost.
- Schedule the evaluation and bring your insurance card, ID, and any relevant records.
- At the first visit, ask how progress will be measured over the next 2-4 weeks.
Your first PT visit usually includes history, movement testing, ROM, strength assessment, gait or balance testing if needed, and a home exercise plan. A common home program for lumbar stiffness or mild back-related mobility loss may start with the following, if your therapist says it fits your condition:
- Lie on your back with knees bent and feet flat.
- Tighten your lower abdomen gently without holding your breath for 5 seconds.
- Perform 10 repetitions.
- Then pull one knee toward your chest, hold 10 seconds, switch sides, repeat 5 times each.
- Stand and walk for 3-5 minutes at an easy pace.
- Repeat 1-2 times per day unless the movement clearly increases leg symptoms.
For shoulder stiffness, a basic early routine may include pendulum swings for 30-60 seconds, wall slides for 10 repetitions, and scapular retraction holds for 10 repetitions, but only after the therapist confirms the diagnosis. The right exercise depends on the tissue involved. Rotator cuff overload, adhesive capsular stiffness, and cervical referral patterns are not managed the same way.
Seek urgent care rather than routine scheduling if you have rapidly worsening weakness, loss of bowel or bladder control, severe head injury symptoms, new seizure activity, or sudden neurologic changes. Routine PT is appropriate when your main problem is pain with movement, reduced ROM, weakness, gait change, balance deficit, or loss of function without emergency red flags.
The practical move is straightforward: find a physical therapist near you, verify your Medicare coverage before the appointment, and ask for a clear plan of care built around measurable function.
Frequently Asked Questions
Does Medicare cover physical therapy in Georgia for back pain?
Medicare may cover PT for back pain in Georgia if the treatment is medically necessary and tied to measurable functional limits such as poor walking tolerance, limited trunk ROM, difficulty with stairs, or weakness affecting daily activity. General wellness visits are not the same as skilled PT.
How long does Medicare pay for physical therapy?
There is not a simple fixed number of visits that applies to every patient. Medicare generally pays while the therapy remains medically necessary and documentation supports skilled treatment. A mild condition may need 4-6 visits. A more complex gait or balance problem may need 8-12 weeks of care with periodic reassessment.
Do I need a referral for physical therapy with Medicare?
You may not always need a referral just to be seen, but the billing process usually requires an evaluation and a certified plan of care for covered treatment. If you have a Medicare Advantage plan, referral and authorization rules may be stricter.
What counts as medically necessary physical therapy?
Medically necessary PT usually means you have a documented functional problem that requires a therapist’s skill. Examples include reduced knee extension affecting gait, weak hip abductors causing instability, limited shoulder ROM affecting dressing, or balance deficits increasing fall risk.
Why did Medicare deny physical therapy?
Common reasons include missing certification of the plan of care, poor documentation of functional deficits, lack of progress reporting, provider network issues, or missing authorization with Medicare Advantage. Ask the practice for the exact denial reason and whether a corrected claim is being submitted.
When should I start physical therapy after an injury?
For many non-emergency musculoskeletal injuries, starting PT within 1-2 weeks helps reduce stiffness and restore movement patterns. If you have major weakness, severe neurologic symptoms, head injury red flags, or sudden loss of function, seek urgent medical evaluation first.