Rotator Cuff Tears: What Patients Need to Know: a rotator cuff tear is a strain or split in one or more shoulder tendons that help lift, rotate, and stabilize your arm. The tear may be small and painful only with certain movements, or larger and cause weakness when you raise the arm.
The rotator cuff includes the supraspinatus, infraspinatus, teres minor, and subscapularis. These muscles attach the shoulder blade, or scapula, to the upper arm bone, or humerus, and keep the humeral head centered in the shoulder socket during reaching, lifting, dressing, pushing, and sleeping positions.
What Is a Rotator Cuff Tear?
A rotator cuff tear occurs when one of the shoulder tendons frays, splits, or pulls away from its attachment on the humeral head. The supraspinatus tendon is the most commonly involved because it passes under the acromion and works hard during arm elevation.
The shoulder has more motion than any other major joint, but that mobility comes with a stability cost. The rotator cuff compresses the humeral head into the glenoid, while larger muscles such as the deltoid, pectoralis major, trapezius, and latissimus dorsi move the arm. When the cuff fails to control the joint, the shoulder can pinch, ache, or lose strength.
Clinical imaging studies show rotator cuff tears become more common with age, especially after age 50, even when pain is mild or intermittent.
Common structures involved in rotator cuff pain include:
- Supraspinatus tendon: often painful with lifting the arm out to the side.
- Infraspinatus tendon: commonly weak with outward shoulder rotation.
- Subscapularis tendon: involved when reaching behind the back becomes weak or painful.
- Subacromial space: the narrow area under the acromion where tendons can become irritated.
- Biceps tendon: often contributes to front-of-shoulder pain when cuff mechanics change.
Rotator cuff tears are different from general shoulder soreness. Pain location, weakness pattern, loss of ROM, and response to loading help a chiropractor, physical therapist, or rehabilitation provider decide the next step.
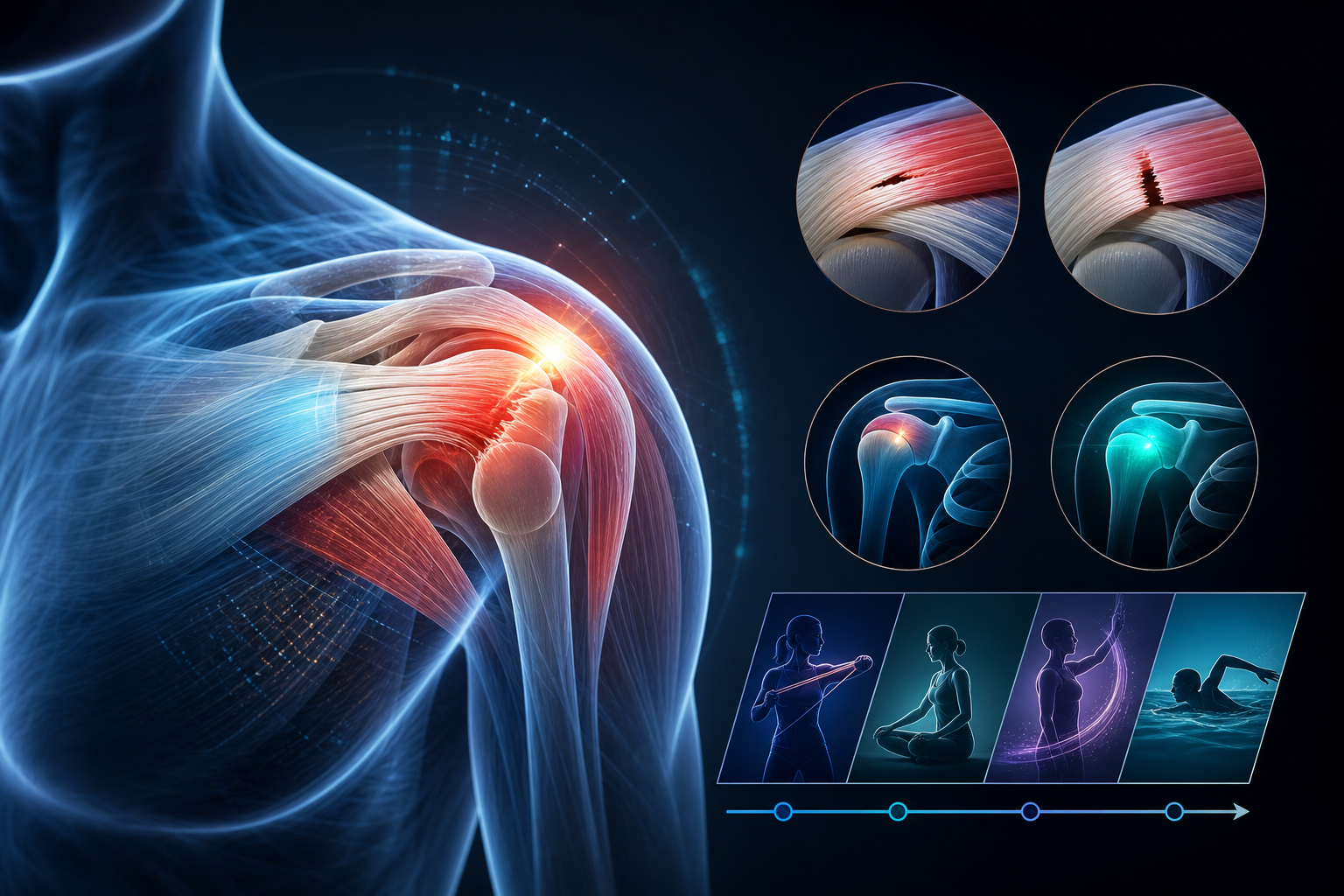
What Is the Difference Between Partial and Full Thickness Rotator Cuff Tears?
The difference between partial and full thickness rotator cuff tear findings is depth. A partial tear affects part of the tendon thickness; a full thickness tear extends through the tendon from top to bottom.
Partial-Thickness Tears
A partial-thickness tear means some tendon fibers remain intact. You may still lift the arm, but pain usually increases between 60 and 120 degrees of elevation, during overhead reaching, or when lowering a weight from shoulder height.
A partial tear can involve the bursal side, articular side, or inside substance of the tendon. Small partial tears often respond well to load management, scapular control work, and progressive rotator cuff strengthening over 6-12 weeks.
Full-Thickness Tears
A full-thickness tear passes through the entire tendon. Some people can still lift the arm by using the deltoid, upper trapezius, and shoulder blade muscles, but strength usually drops with resisted external rotation, abduction, or reaching away from the body.
Useful differences include:
- Partial tear: pain with certain angles, preserved strength, slower onset in many cases.
- Full thickness tear: more obvious weakness, difficulty lifting away from the side, possible catching or shoulder shrug compensation.
- Large tear: difficulty lifting the arm after a fall, visible weakness, or inability to hold the arm up.
Rotator Cuff Tear vs. Tendinitis: How Can You Tell?
Rotator cuff tear vs tendinitis how to tell: tendinitis usually means irritated tendon tissue without a structural split, while a tear means tendon fibers have separated. Both can cause pain with reaching, lifting, and sleeping on the shoulder.
Rotator cuff tendinitis often develops after a spike in activity: painting, lifting boxes, starting a new gym program, or doing repeated overhead work. Pain may be sharp during movement but strength often returns when pain decreases. A tear is more likely when weakness persists even after the pain calms down.
The distinction is not always obvious from symptoms alone. Orthopedic tests such as empty can, external rotation lag, lift-off, drop arm, and resisted abduction help screen the cuff, but imaging such as MRI or diagnostic ultrasound may be needed when weakness is significant or symptoms do not improve.
Feature Tendinitis Rotator Cuff Tear Pain onset Often gradual after repetitive loading Can be sudden after injury or gradual with degeneration Strength Usually limited mainly by pain May remain weak even when pain is controlled ROM Often painful but available Active ROM may be limited more than passive ROM Typical early care Activity modification, soft tissue work, mobility, graded loading Same foundation, with closer strength tracking and functional testingNeck mechanics can mimic or amplify shoulder symptoms. If pain travels from the neck into the shoulder blade or arm, review what patients should know about neck injuries and discuss cervical screening during your visit.
What Causes Rotator Cuff Tears in Older Adults and Active People?
Rotator cuff tears usually come from one of three patterns: acute injury, repetitive overhead loading, or age-related tendon degeneration. The same shoulder can have more than one cause.
Acute Injuries
An acute tear can happen after falling on an outstretched arm, catching a heavy object, pulling hard against resistance, or lifting a load away from the body. Sudden weakness after a fall deserves prompt evaluation, especially if you cannot raise the arm above shoulder height.
Repetitive Overhead Activity
Repeated reaching narrows the subacromial space and increases load on the supraspinatus and infraspinatus. Painters, electricians, warehouse workers, swimmers, tennis players, and baseball athletes often develop cuff irritation when training volume rises faster than tendon capacity.
Age-Related Degeneration
What causes rotator cuff tears in older adults is usually tendon wear plus reduced tissue recovery capacity. Blood flow to parts of the cuff is limited, collagen quality changes with age, and bone shape around the acromion can increase mechanical stress.
Risk factors include:
- Age over 50, especially with years of overhead work.
- Prior shoulder injury or repeated flare-ups.
- Poor scapular control, especially excessive shoulder shrugging during arm elevation.
- Thoracic spine stiffness that forces more motion through the shoulder joint.
- High weekly training volume without recovery days.
- Neck or upper rib restrictions that alter shoulder blade motion.
Shoulder mechanics do not stop at the shoulder. Upper cervical and thoracic alignment can affect muscle tone through the trapezius, levator scapulae, and serratus anterior; this is one reason some patients with shoulder pain also benefit from learning what upper cervical subluxation means in a chiropractic evaluation.
What Does a Rotator Cuff Tear Feel Like?
What does a rotator cuff tear feel like: most people report pain on the outside or front of the shoulder, weakness when lifting the arm, pain reaching behind the back, and shoulder pain at night. Pain may travel toward the upper arm but usually does not pass below the elbow unless the neck or a nerve is involved.
Can you lift arm with rotator cuff tear? Often, yes. Many partial tears still allow arm elevation, especially if the deltoid and shoulder blade muscles compensate. A larger tear may cause a shoulder shrug pattern, dropping of the arm, or inability to control the arm while lowering it.
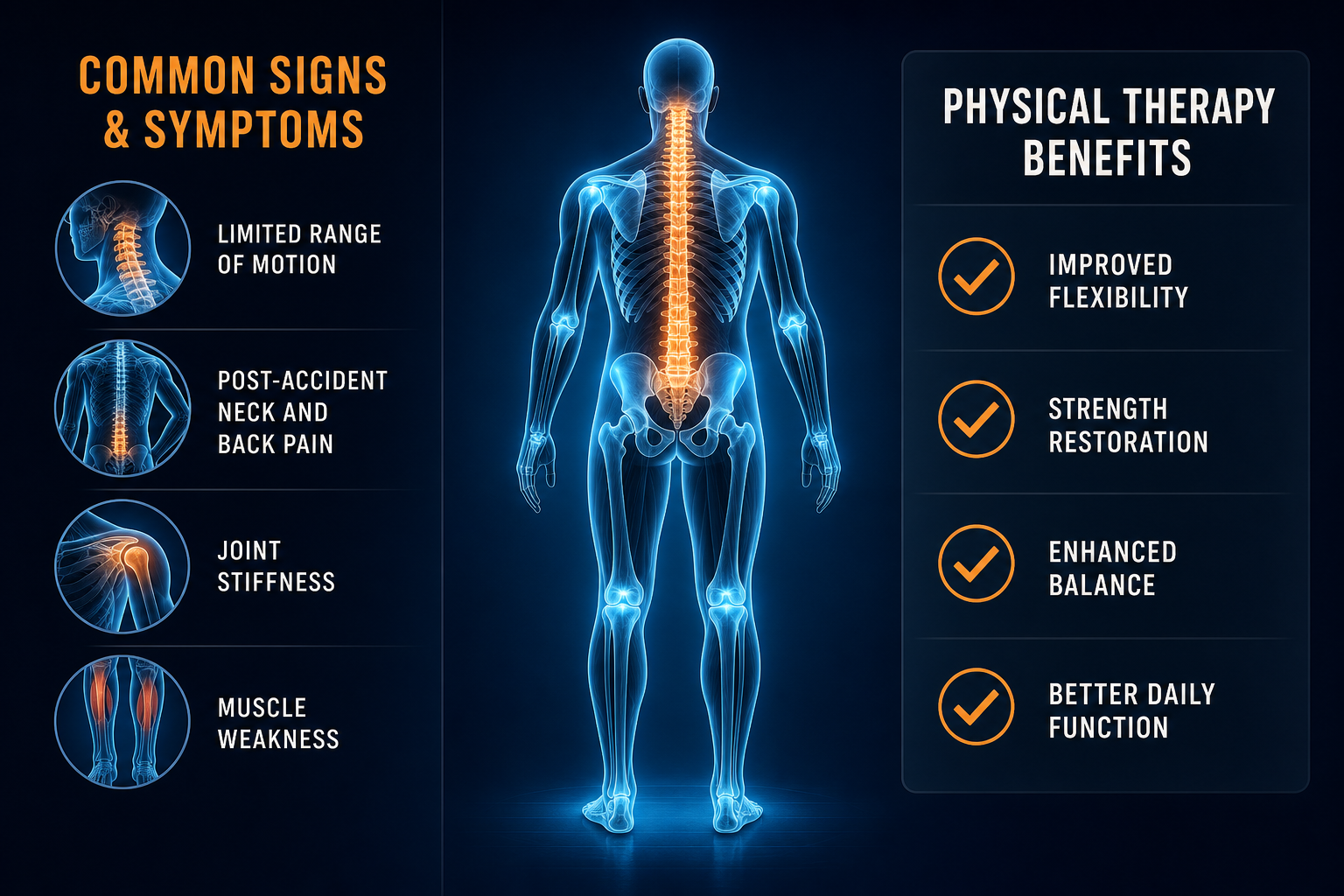
Symptoms to track before your visit:
- Pain reaching into a cabinet, putting on a jacket, or fastening clothing behind the back.
- Weakness during outward rotation, such as opening a heavy door or reaching for a seatbelt.
- Painful arc between shoulder height and overhead range.
- Shoulder pain at night, especially when lying on the painful side.
- Clicking, catching, or a sense that the shoulder does not track smoothly.
- Loss of active ROM compared with the other side.
Seek urgent care now if shoulder pain follows a major fall, collision, or accident and you notice deformity, numbness, spreading weakness, chest pressure, shortness of breath, fainting, fever, or inability to move the arm. After a head or neck impact, review what to do after a possible concussion and get evaluated promptly.
When Should You See a Provider for Shoulder Rotator Cuff Pain?
See a provider when shoulder pain lasts more than 7-10 days, interrupts sleep for several nights, causes measurable weakness, or limits work, lifting, dressing, driving, or exercise. Earlier evaluation is appropriate after trauma or when active arm elevation drops suddenly.
When to see provider for shoulder rotator cuff pain depends on function, not pain score alone. A mild ache with full strength can often start with short-term activity changes. A painful shoulder with weakness, night pain, and poor overhead control should be assessed.
A practical rule: if you cannot raise the arm to shoulder height without shrugging after 72 hours of rest and gentle motion, schedule an evaluation.
Use this decision guide:
- Manage briefly at home: mild soreness, full strength, full ROM, symptoms under 1 week, no injury.
- Schedule routine care: symptoms over 7-10 days, night pain, painful arc, reduced ROM, recurrent flare-ups.
- Schedule promptly: sudden weakness, fall-related pain, inability to lift the arm, visible bruising, major loss of function.
- Seek emergency care: chest symptoms, severe trauma, arm numbness with spreading weakness, deformity, fever, or signs of stroke.
If you want shoulder-focused conservative care, you can find a chiropractor near you or find a physical therapist near you through Medximity. For related foot and lower-limb rehab principles, see how chiropractic care may support plantar fasciitis recovery.
Which Conservative Treatments Help Rotator Cuff Tears?
Conservative care for rotator cuff tears focuses on reducing overload, restoring shoulder ROM, improving scapular mechanics, strengthening the remaining cuff fibers, and returning to normal lifting in phases. A partial rotator cuff tear often improves with this plan when load progression is specific and consistent.
Chiropractic Care
Chiropractic care may address cervical spine, thoracic spine, rib, and shoulder joint mobility that affects shoulder mechanics. Treatment may include spinal manipulation, shoulder mobilization, soft tissue therapy, posture training, and corrective exercise for the rotator cuff and scapular stabilizers.
Physical Therapy
Physical therapy usually emphasizes objective strength testing, ROM restoration, isometrics, eccentric loading, closed-chain shoulder control, and return-to-task training. Programs often progress from pain-limited motion to resisted external rotation, rows, scaption raises, and overhead tolerance work.
Dry Needling and Soft Tissue Therapy
Dry needling may target trigger points in the infraspinatus, upper trapezius, posterior deltoid, or pectoralis minor when muscle guarding limits motion. Soft tissue therapy can reduce stiffness in the posterior cuff, latissimus dorsi, pec minor, and upper thoracic region.
Common conservative treatment options include:
Treatment Primary Goal Expected Outcome Typical Timeline Activity modification Reduce tendon overload Less night pain and fewer sharp symptoms 1-3 weeks Shoulder and thoracic mobility Improve ROM and mechanics Easier reaching and less compensation 2-6 weeks Rotator cuff strengthening Improve tendon capacity Better lifting, reaching, and arm control 6-16 weeks Scapular stabilization Improve shoulder blade control Less shrugging and smoother overhead movement 4-12 weeks Dry needling or soft tissue therapy Reduce guarding and improve movement tolerance Short-term pain relief that supports exercise progression Often reassessed after 2-4 visitsChiropractors and physical therapists often work well together because one provider may focus more on joint mechanics while the other emphasizes progressive loading and functional testing. You can browse providers to compare conservative care options in your area.
Home Exercise Protocol: Pain-Limited External Rotation Isometric
This drill starts cuff activation without heavy joint motion. Stop if pain becomes sharp, spreads, or remains worse for more than 24 hours.
- Stand sideways next to a wall with the affected elbow bent to 90 degrees and tucked against your ribs.
- Place the back of your hand against the wall as if you were trying to rotate the forearm outward.
- Press gently into the wall at 30-50% effort without moving the shoulder.
- Hold 10 seconds while keeping the shoulder relaxed and the neck quiet.
- Repeat 5 times, once or twice daily for 7 days.
- Progress only if pain stays at 0-3 out of 10 during and after the drill.
If symptoms include widespread pain sensitivity or multiple painful regions, the principles in natural care options for fibromyalgia patients may help explain why pacing and graded activity matter.
How Long Does a Rotator Cuff Tear Take to Heal with Conservative Care?
How long does rotator cuff tear take to heal: many mild partial tears improve in 6-12 weeks with consistent conservative care, while larger or long-standing tears may require 3-6 months of progressive strengthening and activity modification.
Tendon tissue adapts slowly. Pain may improve before strength returns, which is why stopping rehab after the first 2-3 better weeks often leads to relapse. A good plan tracks both symptoms and performance: active elevation, external rotation strength, sleep tolerance, work tasks, and lifting capacity.
Strength gains in tendon-related shoulder rehab commonly require at least 8-12 weeks because collagen remodeling and motor control changes lag behind early pain relief.
A typical progression looks like this:
- Week 0-2: reduce painful loads, restore comfortable ROM, start isometrics, improve sleep positioning.
- Week 2-6: add band external rotation, rows, scapular control, thoracic mobility, and light functional reaching.
- Week 6-12: progress resistance, add controlled overhead work if tolerated, train eccentric lowering.
- Month 3-6: return to heavier lifting, sport, or repetitive work demands with task-specific loading.
Setbacks usually come from doing too much too soon: overhead lifting, heavy pressing, sudden yard work, long painting sessions, or sleeping directly on the painful shoulder. Keep pain during exercise at 0-3 out of 10, and make sure symptoms return to baseline by the next morning.
What Happens at the First Chiropractic or Physical Therapy Visit?
A first visit for shoulder pain should identify whether the main driver is the rotator cuff, shoulder joint, neck, upper back, nerve tissue, or a combination. The provider should test ROM, strength, painful arc, shoulder blade control, neck screening, and functional movements that match your daily demands.
If you searched for rotator cuff tear treatment chiropractor near me or first chiropractic visit for shoulder injury what to expect, expect an exam before treatment. A quality visit does not jump straight to a modality; it measures what you can and cannot do.
Common exam components include:
- History of onset, injury mechanism, work demands, sport activity, and sleep position.
- Active and passive ROM testing for flexion, abduction, internal rotation, and external rotation.
- Resisted strength tests for supraspinatus, infraspinatus, subscapularis, biceps, and deltoid.
- Neck screening for cervical radiculopathy when pain travels below the elbow.
- Scapular assessment during arm elevation and lowering.
- Discussion of whether X-ray, MRI, or ultrasound referral is appropriate based on weakness and history.
Your first care plan should include a working diagnosis, activity limits, 1-3 home exercises, expected visit frequency, and measurable goals. Many uncomplicated cases start with 1-2 visits per week for 3-6 weeks, then taper as home loading improves.
Shoulder and neck symptoms often overlap. If headaches, neck stiffness, or upper cervical symptoms accompany shoulder pain, learn common causes of head pain and mention those symptoms during the exam.
Frequently Asked Questions About Rotator Cuff Tears
Can a rotator cuff tear improve with conservative care?
Yes. Many partial tears and some full-thickness tears improve with activity modification, physical therapy, chiropractic care, and progressive strengthening. Improvement depends on tear size, age, strength loss, symptom duration, and daily shoulder demands.
How do I know if I tore my rotator cuff?
A tear is more likely when shoulder pain comes with weakness, painful overhead lifting, night pain, difficulty reaching behind the back, or a drop-arm pattern. A provider can test strength and ROM, then refer for imaging if needed.
What makes a rotator cuff tear worse?
Heavy overhead lifting, repeated reaching, sleeping on the painful side, sudden pulling, poor scapular control, and pushing through sharp pain can increase symptoms. Tendons respond best to graded loading, not complete rest or aggressive overload.
Is it safe to exercise with a rotator cuff tear?
Exercise is usually appropriate when pain stays mild and strength work is controlled. Start with isometrics and pain-free ROM. Avoid heavy overhead pressing, fast throwing, dips, and loaded end-range positions until cleared by your provider.
How long does a rotator cuff tear take to heal?
Mild partial tears often improve in 6-12 weeks. Larger, chronic, or full-thickness tears may require 3-6 months of structured conservative care to regain strength and function. Timelines vary by tear size and activity demands.
Can shoulder pain at night mean a rotator cuff tear?
Yes. Night pain is common with rotator cuff tears, tendinitis, and shoulder joint irritation. If night pain lasts more than several nights or comes with weakness, schedule an evaluation.
What to Do Next
Schedule an evaluation if shoulder pain lasts longer than 7-10 days, limits lifting, disrupts sleep, or causes weakness when raising the arm. Seek urgent care for major trauma, deformity, chest symptoms, fever, spreading numbness, or inability to move the arm after injury.
Choose the provider based on your main limitation:
- Chiropractor: useful when shoulder pain is linked with neck stiffness, upper back restriction, rib mobility, posture, or joint mechanics.
- Physical therapist: useful when you need progressive strengthening, work conditioning, sport return, ROM restoration, and objective strength tracking.
- Rehabilitation provider: useful when pain has lasted months, multiple areas contribute, or you need a staged return-to-activity plan.
At the first visit, bring a list of painful movements, your work or sport demands, how long symptoms have been present, and any prior X-ray or MRI report. Expect testing of the rotator cuff, scapula, cervical spine, thoracic spine, and functional reaching patterns.
To start conservative care, find a shoulder pain provider near you. You can also explore more health topics on Medximity before your visit.
This article is for educational purposes only and does not replace an evaluation from a licensed healthcare provider. Seek emergency care for severe trauma, chest symptoms, stroke-like symptoms, fever, deformity, or rapidly worsening weakness.