If you have ever felt a sharp, burning, or electric sensation radiating from your lower back down through your buttock, leg, or foot, you may be experiencing lumbar radiculopathy — a condition caused by irritation or compression of one or more nerve roots in the lower spine. It is one of the most common reasons patients seek conservative care, and the good news is that many people recover well without surgery when the condition is identified early and managed appropriately.
This article explains what lumbar radiculopathy is, what causes it, how it is diagnosed, and what your treatment options look like — including chiropractic care and physical therapy — so you can have a productive conversation with a provider and feel confident about next steps.
What Is Lumbar Radiculopathy?
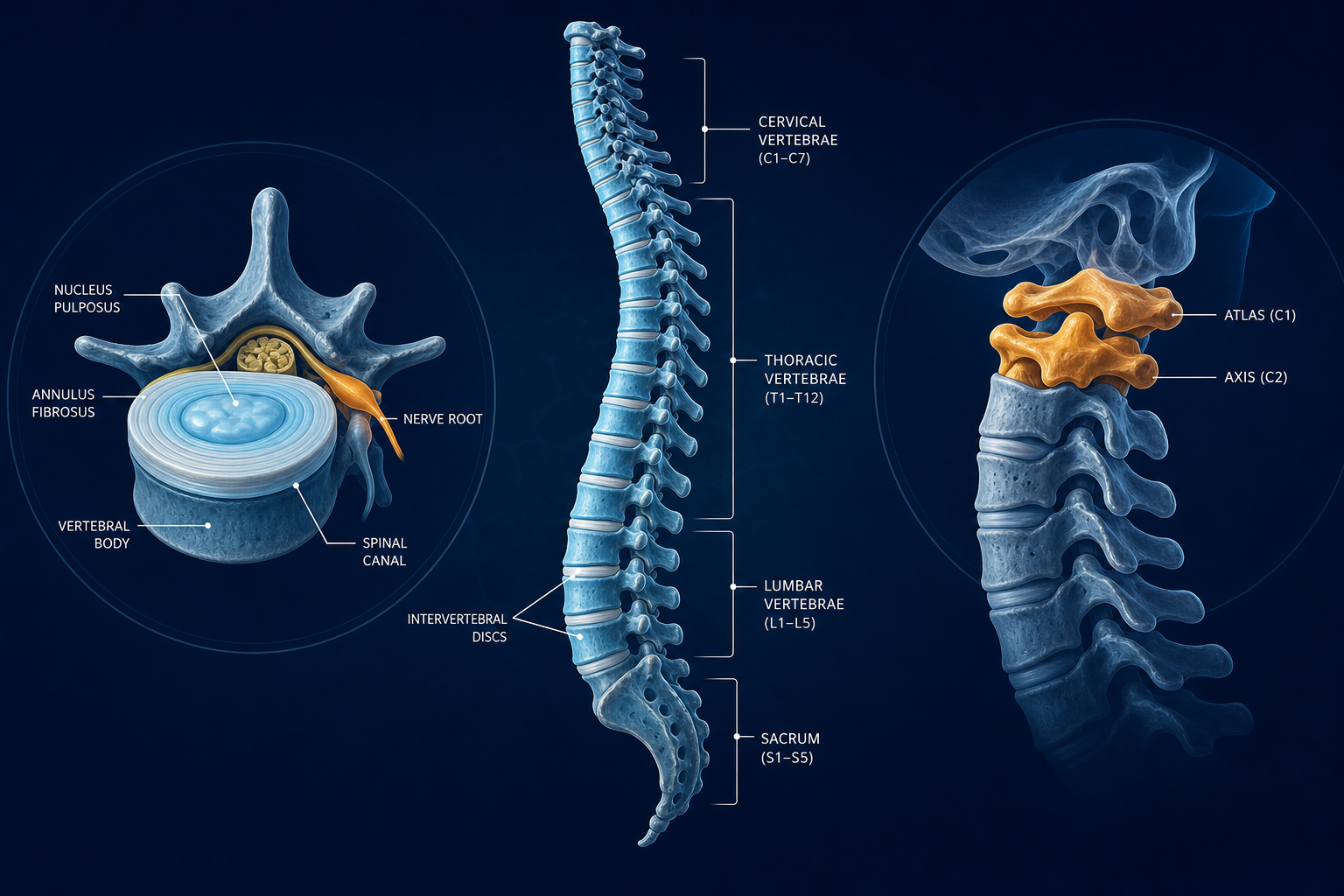
Lumbar radiculopathy occurs when a nerve root in the lumbar spine — the lower portion of your backbone, roughly from your waistline to your tailbone — becomes compressed, inflamed, or chemically irritated where it exits the spinal column. The lumbar spine contains five vertebrae (L1 through L5), and the sacrum sits just below. Nerve roots at each level travel outward and downward, eventually forming the large nerves that supply sensation and muscle control to your legs and feet.
When one of those roots is pinched or inflamed, pain, tingling, numbness, or weakness can radiate along the path of that nerve — a phenomenon called radicular pain, from the Latin word for root. The specific symptoms and where they travel depend largely on which nerve root is affected.
Is Lumbar Radiculopathy the Same as Sciatica?
These two terms are often used interchangeably, but there is a meaningful difference between sciatica and lumbar radiculopathy. Sciatica is a symptom — specifically, pain that follows the path of the sciatic nerve, which is formed by nerve roots from L4 through S1 and runs down the back of the thigh and calf. Lumbar radiculopathy is a broader clinical diagnosis that describes nerve root involvement at any lumbar level, which may or may not produce the classic sciatic pattern. In practice, L4, L5, and S1 radiculopathy account for the majority of cases, and those almost always produce symptoms that fit the everyday description of sciatica. But radiculopathy at L2 or L3, for example, may instead cause pain in the groin or the front of the thigh — patterns that patients and even some providers may not immediately recognize as a nerve root problem.
What Causes Lumbar Radiculopathy?
Several underlying conditions can compress or irritate a lumbar nerve root. The most common causes include:
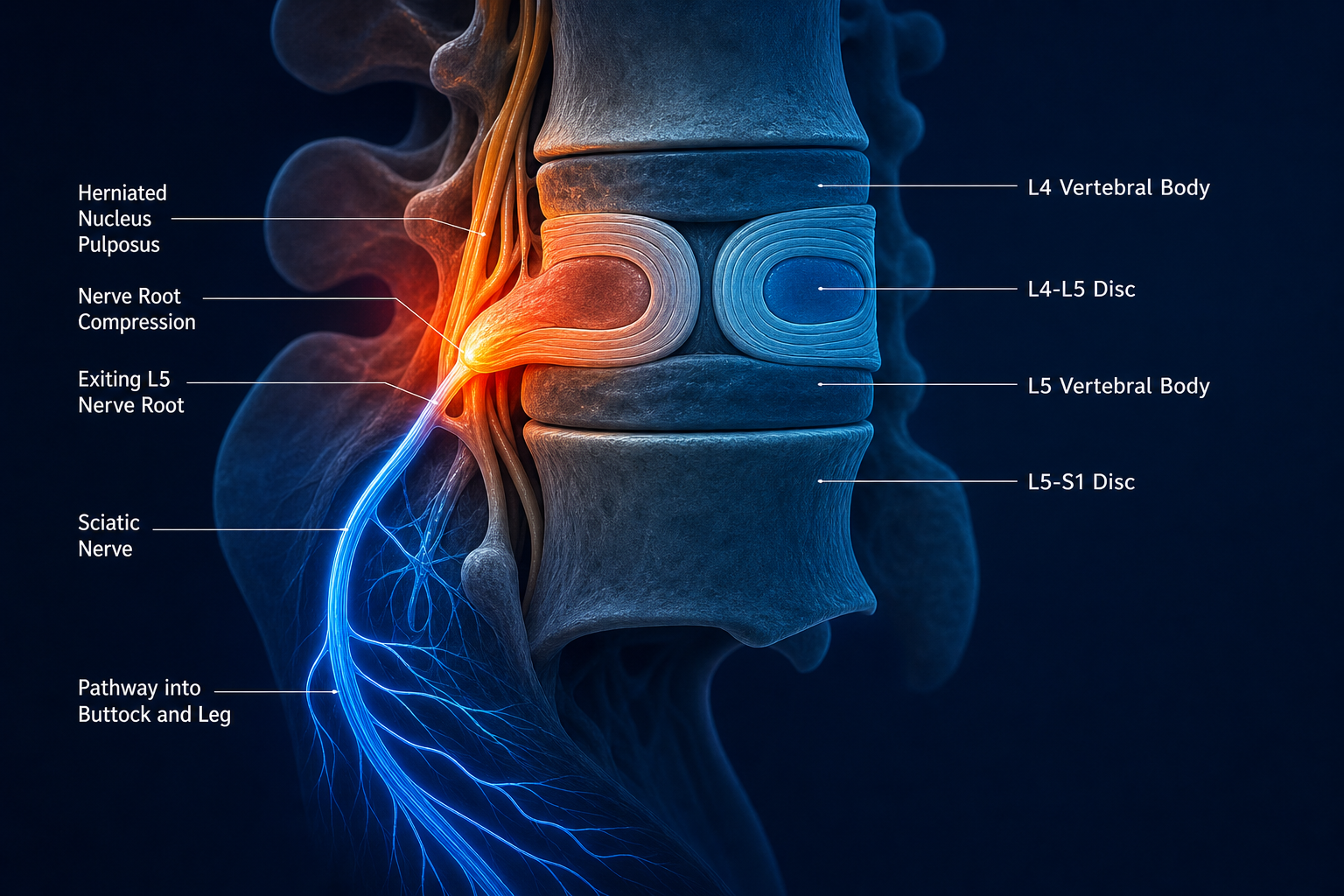
- Disc herniation: The gel-like nucleus inside an intervertebral disc can bulge or rupture outward, pressing directly on an adjacent nerve root. This is the most frequent cause in patients under 50.
- Degenerative disc disease and bone spurs: As discs lose height and flexibility over time, bone spurs (osteophytes) can develop and narrow the openings through which nerve roots exit — a process called foraminal stenosis.
- Lumbar spinal stenosis: A narrowing of the spinal canal itself, often from a combination of disc changes, ligament thickening, and joint arthritis. More common in older adults.
- Spondylolisthesis: A condition where one vertebra slips forward relative to the one below it, potentially pinching nerve roots in the process.
- Acute injury: A fall, motor vehicle accident, or heavy lifting incident can acutely herniate a disc or cause vertebral changes that immediately compress a nerve root.
Chemical irritation also plays a role. When a disc is damaged, inflammatory proteins can leak out and irritate nearby nerve tissue even without direct mechanical compression — which is part of why nerve pain can feel disproportionately intense relative to what imaging reveals.
Recognizing the Symptoms: Nerve Pain Shooting Down the Leg
The hallmark of lumbar radiculopathy is pain that radiates — moves outward from the spine along a predictable nerve pathway — rather than staying localized to the lower back. Patients often describe the sensation as burning, electric, stabbing, or sharp. Some describe it as a deep ache that is hard to escape regardless of position.
Common symptoms include:
- Shooting or burning leg pain that may extend into the calf or foot
- Numbness or tingling in the leg, ankle, or specific toes
- Muscle weakness in the leg or foot — difficulty raising the foot (foot drop) is a particularly important finding
- Pain that worsens with sitting, coughing, sneezing, or straining
- Relief in certain positions, such as lying down with knees bent
If you are asking yourself is it normal to have leg pain with a lower back injury — the answer is yes, it is common, but it deserves evaluation. Leg pain following a back injury may signal nerve root involvement, and understanding whether that is the case shapes the entire treatment approach.
Red Flag Symptoms That Require Immediate Attention
Most lumbar radiculopathy is uncomfortable but not dangerous. However, certain symptoms suggest a more serious neurological emergency. Seek urgent medical evaluation if you experience:
- Loss of bowel or bladder control, or sudden difficulty urinating
- Numbness or tingling in the groin or inner thighs (saddle anesthesia)
- Rapidly progressing weakness in one or both legs
- Severe symptoms following significant trauma such as a car accident or fall from height
- Unexplained weight loss, fever, or history of cancer alongside new back and leg pain
These red flag symptoms may indicate cauda equina syndrome or another condition requiring emergency intervention. Do not wait for a scheduled appointment if they are present.
Lumbar Radiculopathy Treatment Without Surgery
For the majority of patients, lumbar radiculopathy responds well to conservative, non-surgical treatment. Research consistently suggests that most cases — particularly those caused by disc herniation — improve significantly within weeks to a few months with appropriate care. Here is what evidence-informed conservative management typically looks like.
Chiropractic Care for Lumbar Radiculopathy
Chiropractors are trained to evaluate the spine and musculoskeletal system and are frequently the first conservative-care provider patients see for nerve root pain. Chiropractic management for lumbar radiculopathy may include:
- Spinal manipulation and mobilization: Gentle, controlled forces applied to lumbar segments may help restore movement, reduce joint restriction, and decrease nerve root irritation. Technique selection depends on the individual's presentation, and many chiropractors use lower-force approaches when radiculopathy is involved.
- Flexion-distraction technique: A specialized table-based technique that gently decompresses lumbar discs and nerve roots without high-velocity thrusting. Commonly used for disc-related radiculopathy.
- Soft tissue therapies: Myofascial release and trigger point work targeting muscles that may be guarding and contributing to nerve tension.
- Postural and ergonomic counseling: Guidance on positions that reduce nerve root loading during the acute phase.
If you are searching for chiropractic care for lumbar radiculopathy near you, Medximity's provider directory lets you search by location and specialty to find credentialed chiropractors in your area.
Physical Therapy for Lumbar Radiculopathy
Physical therapy focuses on restoring movement, building strength in the muscles that support the lumbar spine, and reducing the mechanical load on irritated nerve roots. A physical therapist will typically conduct a detailed movement assessment before designing a program specific to your nerve root level and functional limitations.
Common physical therapy interventions include:
- McKenzie Method (mechanical diagnosis and therapy): A directional exercise approach that identifies specific movements — often extension-based — that centralize radicular symptoms, meaning pain moves from the foot back toward the spine, which is generally a positive prognostic sign.
- Nerve mobilization (neurodynamic techniques): Gentle movements designed to restore the normal gliding and tensioning of the sciatic or other affected nerve along its path.
- Core stabilization exercises: Targeted strengthening of the deep abdominal and lumbar muscles that help protect nerve roots from further irritation.
- Traction: Manual or mechanical traction may reduce compressive forces on a herniated disc and associated nerve root in select patients.
When comparing physical therapy vs. chiropractic for a pinched nerve in the back, the honest answer is that both have demonstrated value, they address overlapping and complementary aspects of the problem, and many patients benefit from a collaborative approach. The right choice — or combination — depends on your specific diagnosis, imaging findings, functional goals, and provider availability. Find a physical therapist near you through Medximity's directory.
Exercises for Lumbar Radiculopathy Nerve Root Pain
Exercise is a cornerstone of recovery, but the specific exercises that help versus hurt depend on which nerve root is involved and the underlying cause. Self-directed exercise without a professional assessment carries some risk of worsening symptoms during the acute phase. That said, gentle movement is almost always better than complete bed rest, which evidence suggests may actually slow recovery.
A provider may guide you through movements such as prone press-ups (McKenzie extension), pelvic tilts, supine knee-to-chest stretches, and nerve gliding sequences. Always begin any exercise program under the guidance of a licensed provider who has evaluated your specific presentation.
Learn more about how movement supports spine recovery in our related article: Physical Therapy for Lower Back Pain: A Patient's Guide.
How Long Does Lumbar Radiculopathy Take to Heal?
Recovery timelines vary considerably depending on the cause, severity, how quickly care was initiated, and individual factors like age and overall health. As a general picture:
- Mild to moderate disc-related radiculopathy often improves meaningfully within 6 to 12 weeks of consistent conservative care.
- More significant nerve root compression or cases involving motor weakness may take three to six months or longer.
- Cases with prolonged nerve compression — particularly those involving foot weakness or numbness — may see gradual, incremental improvement over many months, as nerve tissue heals more slowly than muscle or soft tissue.
Progression is not always linear. Many patients have better days and setbacks. The goal of conservative care is not to eliminate all discomfort overnight but to restore function, reduce nerve irritation, and prevent recurrence.
Can Lumbar Radiculopathy Cause Foot Weakness and Numbness?
Yes — and this is one of the more concerning presentations. The L4, L5, and S1 nerve roots control specific muscle groups in the lower leg and foot. Compression of L5, for instance, may cause weakness in the muscles that lift the front of the foot (ankle dorsiflexion), resulting in foot drop — a difficulty clearing the foot during walking. S1 compression may weaken the calf muscles and reduce the Achilles tendon reflex. Numbness in specific areas of the foot often corresponds to the sensory distribution of the affected root.
Foot weakness and significant numbness are important findings that should prompt prompt evaluation. While they do not automatically indicate a surgical emergency, they signal more significant nerve root involvement and may influence how aggressively conservative treatment is pursued.
For more on how nerve injury presents in the lower extremity, see our related article: Sciatica: Symptoms, Causes, and Conservative Treatment Options.
Documenting Your Symptoms for an Insurance Claim
If your lumbar radiculopathy developed after a motor vehicle accident, a workplace incident, or another injury event, thorough documentation of your symptoms is important for any insurance or legal process. While documentation strategy is ultimately a matter to discuss with a licensed attorney who knows your jurisdiction, providers play a critical role by creating detailed clinical records that accurately reflect your condition over time.
As a patient, you can support this process by:
- Seeking evaluation promptly after an injury rather than waiting to see if symptoms resolve on their own
- Describing your symptoms in detail at each visit — location, quality, intensity, what makes them worse or better, and how they affect your daily activities
- Attending all scheduled appointments consistently, since gaps in care can complicate claims
- Keeping a personal symptom journal noting daily pain levels, functional limitations, and missed activities
Providers using integrated documentation systems — like Digital Patient Chart, the EHR built for chiropractic and rehabilitation practices — create visit records that are structured, time-stamped, and medically detailed, which tends to support the kind of documentation injury cases require. If you are working with an attorney on a personal injury matter, they can advise you on what records to request and how documentation supports your specific claim. Laws and procedures vary by state, so jurisdiction-specific legal guidance is essential.
You can also explore how chiropractic documentation supports injury cases in our article: How Chiropractic Records Support Personal Injury Claims.
Finding a Provider for Lumbar Radiculopathy
Conservative care for lumbar radiculopathy works best when it starts early, is guided by a provider who understands nerve root anatomy and mechanics, and is tailored to your specific nerve level and functional presentation. Whether you begin with a chiropractor, a physical therapist, or your primary care provider, the most important step is getting a thorough evaluation so that your treatment is matched to what is actually causing your symptoms.
Use the Medximity provider directory to search for chiropractors and physical therapists in your area who have experience treating lumbar radiculopathy and related conditions. Profiles include specialty focus areas, accepted insurance, and location information to help you find the right fit.
Frequently Asked Questions About Lumbar Radiculopathy
What is the difference between sciatica and lumbar radiculopathy?
Sciatica is a specific symptom pattern — pain along the sciatic nerve, typically down the back of the leg — while lumbar radiculopathy is a clinical term for nerve root irritation or compression at any lumbar level. Sciatica is usually the result of lumbar radiculopathy at L4, L5, or S1, so the terms often overlap, but radiculopathy at higher lumbar levels produces different symptom patterns.
Can lumbar radiculopathy heal without surgery?
Many cases resolve with conservative treatment alone. Research suggests a significant proportion of disc-related radiculopathy improves within weeks to months with chiropractic care, physical therapy, activity modification, and time. Surgery is generally considered when conservative treatment has not produced adequate improvement after an appropriate trial, or when there is significant or progressive neurological deficit.
How long does it take to recover from lumbar radiculopathy?
Recovery varies by cause and severity. Mild cases may improve meaningfully within six to twelve weeks of consistent conservative care. More significant nerve root involvement, or cases with motor weakness, may require several months. Nerve tissue heals more slowly than muscle or soft tissue, so patience and consistent treatment are important.
Is foot numbness or weakness a sign of something serious?
Foot weakness and numbness can indicate more significant nerve root compression and should be evaluated promptly. While not automatically an emergency, these findings influence treatment decisions and may suggest the need for imaging. Loss of bowel or bladder control alongside leg symptoms is a medical emergency — seek immediate care.
Should I choose chiropractic care or physical therapy for lumbar radiculopathy?
Both have demonstrated value for lumbar radiculopathy, and many patients benefit from both. Chiropractors often focus on spinal mechanics and joint mobility, while physical therapists emphasize therapeutic exercise, nerve mobilization, and functional rehabilitation. The best approach depends on your specific diagnosis, severity, and goals — and in many cases, a coordinated approach between both disciplines produces the best outcomes.
What activities should I avoid with lumbar radiculopathy?
Positions and activities that increase pressure on the affected nerve root — such as prolonged sitting, heavy lifting with a rounded back, or high-impact activities — are often best avoided during the acute phase. Your provider can give you specific guidance based on which nerve root is involved and what movements centralize or peripheralize your symptoms.
How is lumbar radiculopathy diagnosed?
Diagnosis typically combines a detailed patient history, neurological examination (testing reflexes, muscle strength, and sensation), and orthopedic tests such as the straight leg raise. Imaging — X-ray, MRI, or CT — may be ordered to identify the underlying structural cause when the clinical picture warrants it. Nerve conduction studies and EMG may be used in complex or prolonged cases to assess nerve function more precisely.