Understanding Intervertebral disc disorders with radiculopathy, thoracolumbar region: Symptoms, Causes, and Treatment starts with one practical point: symptoms come from a disc problem near the T12–L1 junction that irritates a nerve root, creating pain, tingling, numbness, or weakness that follows a predictable pattern. Most cases improve with activity modification, targeted rehab, and manual care over 6–12 weeks, but progressive weakness, bowel/bladder changes, or saddle numbness requires urgent evaluation. This guide shows you how to recognize thoracolumbar radiculopathy, what typically causes it, and how chiropractic and physical therapy care is structured.
What is a thoracolumbar disc disorder with radiculopathy?
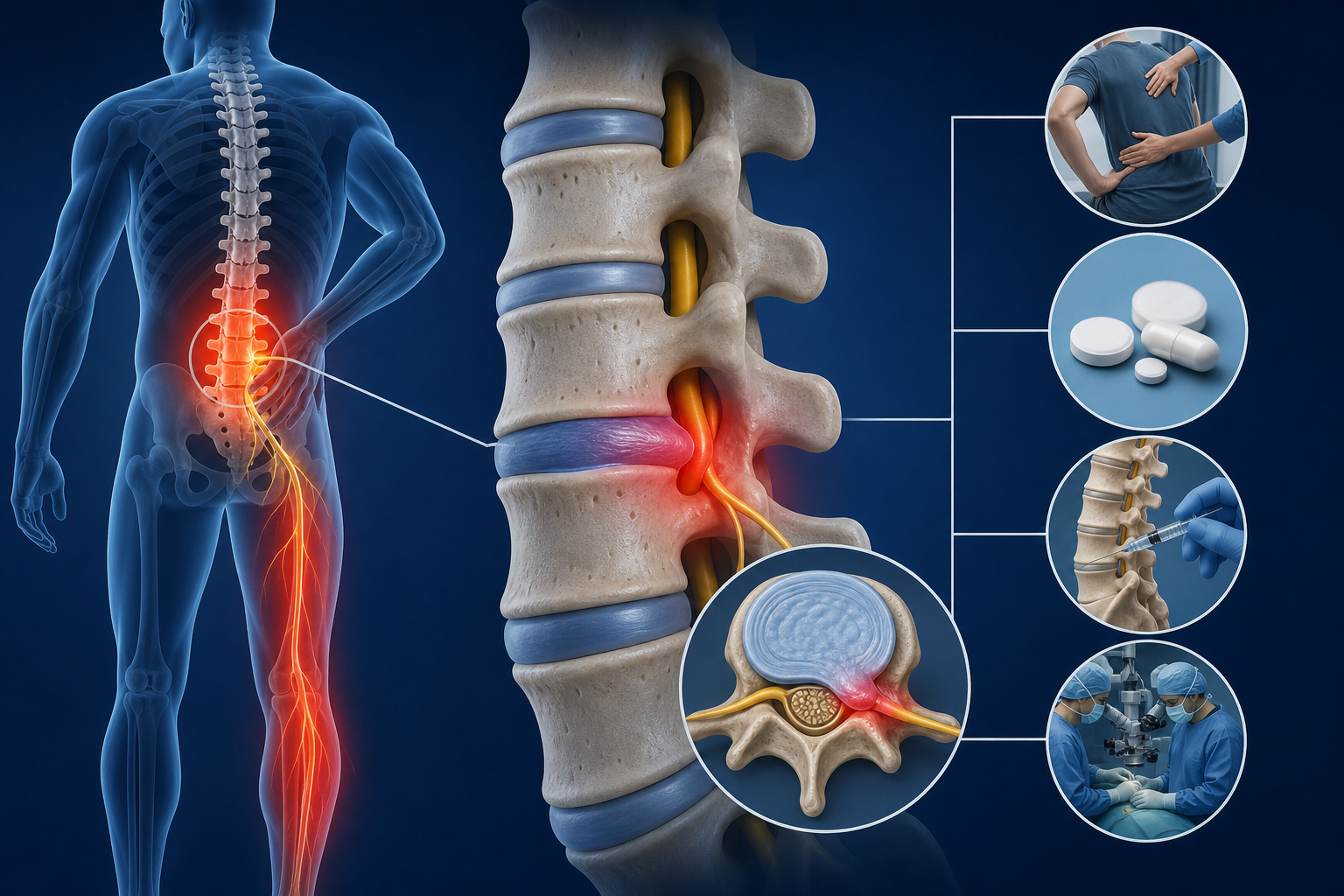
Intervertebral disc disorders with radiculopathy in the thoracolumbar region means a disc at the lower thoracic/upper lumbar junction (commonly T11–T12 or T12–L1) is irritating a nearby nerve root. The disc can bulge or herniate and trigger chemical inflammation and/or mechanical compression around the nerve root as it exits the spine.
The thoracolumbar junction behaves differently than the mid-thoracic spine because it transitions from rib-stabilized thoracic mechanics to more mobile lumbar mechanics. That transition concentrates load during bending, lifting, and rotation.
Key anatomy you should know
- Intervertebral disc: the shock-absorbing disc between vertebrae; the outer ring is the annulus fibrosus and the center is the nucleus pulposus.
- Nerve root: the spinal nerve segment leaving the spinal canal; irritation here creates radicular symptoms (radiating pain, sensory changes, weakness).
- Facet joints: paired joints at the back of the spine that guide motion; stiffness or overload here can amplify pain and limit motion.
- Thoracolumbar fascia: thick connective tissue over the low back that can become sensitized and contribute to protective muscle guarding.
Radiculopathy is different from “referred pain.” Radiculopathy follows a nerve distribution and often changes with spinal position (flexion/extension) and nerve tension tests. The National Institute of Neurological Disorders and Stroke describes radiculopathy as symptoms due to a pinched or irritated nerve root, often from a herniated disc or degenerative changes (NINDS).
What symptoms happen when a disc irritates a nerve at T12–L1?
Thoracolumbar radiculopathy can present as back pain plus symptoms that travel around the trunk or into the hip/groin or upper thigh depending on the level involved. The pattern is less “classic sciatica” and more band-like or flank-to-groin in some cases.
Common symptoms (what you can actually track)
- Radiating pain from the mid-back/low-back junction into the flank, abdomen wall region, groin, or upper buttock/hip.
- Tingling or numbness in a strip-like area around the trunk or into the upper thigh.
- Weakness that shows up as reduced trunk stability, difficulty with hip flexion, or leg fatigue with walking (level-dependent).
- Pain with coughing/sneezing or straining, which can increase pressure around an irritated nerve root.
- Positional sensitivity: worse with sustained flexion (slumped sitting) for many people; others worsen with extension/standing depending on the specific mechanics.
Red flags: get urgent evaluation
- New bowel or bladder control changes.
- Saddle numbness (numbness in the groin/perineal region).
- Rapidly progressive weakness in the leg(s) or repeated falls.
- Fever with severe spine pain or unexplained weight loss.
- Major trauma (fall, car accident) followed by severe pain or neurological symptoms.
If any red flag is present, do not self-treat. Seek urgent care or emergency evaluation.
Most disc-related radicular symptoms improve over time with conservative care; the American Academy of Family Physicians notes that many patients with radicular symptoms recover within several weeks and many disc herniations regress or reabsorb within about 8 weeks (AAFP).
What causes thoracolumbar radiculopathy?
Thoracolumbar radiculopathy is usually driven by disc loading plus tissue sensitivity around the nerve root. A single “bad lift” can trigger symptoms, but more often it is repetitive flexion/rotation, prolonged sitting, deconditioning, or a sudden spike in workload.
- Disc bulge or herniation: the annulus weakens and the nucleus shifts, irritating the nerve root.
- Degenerative disc changes: disc height loss can change foraminal space (the exit tunnel for the nerve root).
- Segmental stiffness above/below the irritated level: restricted thoracic rotation or hip mobility increases torsion at T12–L1.
- Load management issues: fast increases in lifting volume, poor bracing strategy, or fatigue-driven form breakdown.
- Prolonged flexion posture: slumped sitting increases posterior disc pressure in many spines.
Risk rises with smoking, low physical activity, and certain occupational exposures (repetitive lifting, vibration). The NIH/NCBI overview of lumbar disc herniation describes common mechanisms and emphasizes that disc pathology and nerve irritation often coexist (NCBI Bookshelf).
How do you know it’s radiculopathy and not a muscle strain or rib issue?
You separate thoracolumbar radiculopathy from common mimics by combining symptom mapping, neurological screening, and mechanical testing. A muscle strain hurts locally and with contraction/stretch; radiculopathy more often changes with spinal position and produces sensory changes or reflex/strength differences.
Condition Typical pain pattern What changes symptoms Common exam clues Thoracolumbar radiculopathy Back pain + radiating band/flank/groin/upper thigh symptoms Spinal flexion/extension, coughing/sneezing, nerve tension Sensory changes, myotome weakness, positive nerve tension tests (level-dependent) Paraspinal muscle strain Localized ache/spasm near the injury Direct palpation, muscle contraction, stretching Normal neuro screen; pain reproduced with resisted trunk motion Facet joint irritation Local back pain, sometimes referral to buttock/hip Often worse with extension/rotation Pinpoint joint tenderness; limited extension/rotation; neuro screen normal Costovertebral/rib dysfunction Sharp pain near rib angle; pain with deep breath/cough Breathing, trunk rotation, rib springing Reproducible rib tenderness; neuro screen normal- Neurological screen matters: sensation, strength, reflexes, and gait.
- Mechanical preference matters: some people improve with repeated extension (common in disc presentations), others with unloading or neutral spine training.
- Time course matters: a simple strain usually improves noticeably within 7–14 days; persistent radiating symptoms beyond 2–3 weeks increases suspicion for nerve involvement.
If you want a structured triage before booking, use Medximity to check your symptoms and then match to the right provider type.
What treatments work best (and how long do they take)?
Best outcomes come from matching care to your dominant limiter: pain sensitivity, mobility restriction, nerve irritability, or strength/endurance deficits. Conservative care typically targets (1) reducing nerve root irritation, (2) restoring thoracic/hip mobility to unload the junction, and (3) rebuilding trunk endurance so symptoms do not recur with normal life.
Clinical practice guidelines for low back pain support exercise therapy and manual therapy as effective conservative options for many mechanical spine conditions (Journal of Orthopaedic & Sports Physical Therapy).
Typical conservative plan (what it looks like in real weeks)
- Phase 1 (days 1–14): calm symptoms, find positions/movements that centralize pain, limit provocative bending/rotation, begin gentle mobility and isometrics.
- Phase 2 (weeks 2–6): progressive trunk endurance (anti-rotation/anti-extension), hip mobility, graded return to walking and lifting patterns.
- Phase 3 (weeks 6–12): build capacity: loaded carries, hinge patterning, rotational control, sport/work simulation.
Many people notice meaningful improvement by 2–4 weeks when they stop repeatedly provoking the nerve and start a structured progression. If you have true radiculopathy with sensory changes, a more realistic window is 6–12 weeks for stable improvement, with flare-ups decreasing as capacity returns.
Treatment comparison table (expected outcomes and timelines)
Conservative treatment Best for Expected outcome Typical timeline Physical therapy (exercise-based rehab) Weakness, poor trunk endurance, return-to-work/sport planning Improved function, reduced recurrence risk, better lifting tolerance Typically 6–8 visits over 3–6 weeks, then home progression Chiropractic care (manual therapy + rehab) Segmental stiffness, pain with motion, mechanical restriction at thoracolumbar junction Improved ROM, reduced pain, better tolerance for exercise progression Often 4–10 visits over 2–6 weeks depending on irritability Directional preference / McKenzie-style self-management Pain that centralizes with repeated movements Faster symptom control when a clear directional preference exists Often 1–3 weeks to identify and stabilize, then progress Activity and ergonomic modification Symptoms driven by sitting, bending, lifting spikes Fewer flare-ups, better day-to-day control Immediate changes; reassess in 7–10 days Massage / soft-tissue work Protective muscle guarding in paraspinals, QL, gluteals Short-term pain reduction and improved movement tolerance Often 2–6 sessions alongside active rehabIf your goal is the fastest functional return, pair manual care with a progressive home program. Passive care alone rarely holds when you return to lifting, long drives, or desk work.
Which home program helps most? (step-by-step)
A good home program does two jobs: (1) reduce nerve irritability today, and (2) rebuild control around the thoracolumbar junction so the disc is not repeatedly stressed. Use the options below and keep the ones that reduce symptoms within 10–15 minutes and do not worsen symptoms later that day.
Protocol A: “Centralize and calm” (10 minutes, 1–3x/day)
- Unload for 2 minutes: lie on your back with calves on a chair (hips/knees ~90°). Breathe slowly and let the low back relax.
- Prone on elbows (if tolerated) for 2 minutes: lie on your stomach, prop on elbows. Stop if leg symptoms spread farther down the limb.
- Repeated press-ups x 10 reps: from prone, press your chest up while hips stay down. Move within tolerance. Goal: symptoms move toward the spine, not farther away.
- Walk 5 minutes: brisk enough to swing arms. Walking often reduces nerve sensitivity better than stretching.
Protocol B: “Stabilize the junction” (12 minutes, every other day)
- Dead bug ISO: 3 sets of 20–30 seconds. Keep ribs down; do not arch through T12–L1.
- Side plank (knees bent): 3 sets of 15–25 seconds each side. You should feel obliques, not pinching in the spine.
- Hip hinge drill: 2 sets of 10 reps with a dowel along head/upper back/sacrum. Keep all three contact points as you hinge.
- Rule 1: If numbness/tingling spreads farther from the spine during or after the drill, reduce range or stop that drill.
- Rule 2: If pain “centralizes” (moves closer to the spine), you are usually moving in the right direction.
- Rule 3: Avoid aggressive end-range twisting stretches early. Rotation is often the irritant at the thoracolumbar junction.
Expect the home program to change over time. Early goals are symptom control and gentle exposure; later goals are strength, endurance, and load tolerance.
When do you need imaging, and what should you ask your provider?
Most thoracolumbar radiculopathy does not require immediate imaging if symptoms are improving and no red flags exist. Imaging becomes more useful when symptoms persist despite appropriate conservative care, when neurological deficits progress, or when the clinical picture is unclear.
- X-ray helps assess alignment and bony changes but does not show disc herniation directly.
- MRI visualizes discs, nerve roots, and stenosis patterns; it is most helpful when it will change the plan.
Guidelines commonly recommend avoiding early imaging for most non-specific back pain in the absence of red flags because many imaging findings occur in people without symptoms; imaging is most valuable when results will change management (CDC).
Questions that keep your care plan specific
- “Which level do you think is involved: T11–T12, T12–L1, or L1–L2, and why?”
- “Do my symptoms look like nerve root irritation or referred pain from facets/QL?”
- “Which movements should I repeat at home, and which should I avoid for 2 weeks?”
- “What objective measures will we track: ROM, strength, walking tolerance, dermatomal sensation?”
- “What is the checkpoint for escalation if I’m not improving by week 4–6?”
A precise diagnosis is less about a label and more about a reproducible pattern: what positions provoke symptoms, what reduces them, and what deficits show up on a neuro screen.
What to Do Next
Start with a plan that matches symptom severity and neurological findings. If you have red flags (bowel/bladder changes, saddle numbness, rapidly progressive weakness), seek urgent evaluation now.
- For routine care (most cases): book a physical therapy evaluation for a progressive exercise plan and a chiropractic evaluation if you have clear joint restriction or pain with motion that limits rehab.
- What to expect at the first visit: symptom mapping (where pain travels), neuro screen (sensation/strength/reflexes), ROM testing, and a home program you can perform the same day.
- What you should do today: reduce repeated bending/rotation for 7 days, walk daily (start 5–10 minutes), and use Protocol A once or twice daily if it centralizes symptoms.
- Checkpoints: you should see either reduced symptom spread, improved walking tolerance, or improved sleep positioning comfort within 10–14 days. If nothing changes by 3–4 weeks, reassess the diagnosis and plan.
Use Medximity to find a physical therapist near you or find a chiropractor near you. You can also browse providers by specialty and location, and explore more health topics to build a stronger prevention plan once symptoms calm down.
FAQ: Thoracolumbar disc disorders with radiculopathy
How long does thoracolumbar radiculopathy last?
Many cases improve noticeably within 2–4 weeks with activity modification and a targeted home program. If you have sensory changes (numbness/tingling) or measurable weakness, a more typical recovery window is 6–12 weeks, with steady functional gains when you progress walking and trunk endurance.
What movements should you avoid with a thoracolumbar disc problem?
Avoid repeated end-range flexion + rotation (slumped twisting, aggressive toe-touch stretching with rotation) for the first 1–2 weeks if those movements reproduce radiating symptoms. Replace them with neutral-spine hinge mechanics, short walks, and repeated movements that centralize symptoms.
Is thoracolumbar radiculopathy the same as sciatica?
No. Sciatica usually refers to irritation of lower lumbar/sacral nerve roots that travel down the back of the leg. Thoracolumbar radiculopathy more often creates band-like trunk symptoms, flank pain, groin/hip referral, or upper-thigh sensory changes depending on the affected level.
Can chiropractic and physical therapy help a disc bulge with radiculopathy?
Yes, in many cases. Physical therapy targets trunk endurance, hip mobility, graded loading, and return-to-activity planning. Chiropractic care can reduce mechanical restriction and pain that blocks movement and exercise. The best plans combine manual care with a progressive home program and clear checkpoints.
When should you worry about numbness or weakness?
Seek urgent evaluation if numbness spreads rapidly, if you develop new bowel/bladder control changes, saddle numbness, or rapidly progressive weakness. For stable mild numbness without red flags, schedule an evaluation soon and track objective changes (walking tolerance, strength, symptom spread) weekly.